
Shoulder Pain From Exercise: Common Causes and How to Fix Them
This article is for general educational purposes only and does not constitute medical or professional fitness advice.
Stop exercise and consult a healthcare provider if you experience sharp or worsening pain.
Shoulder pain is one of the most common training-related complaints — and one of the most mismanaged, because “shoulder pain” covers a range of very different conditions that respond to different interventions.
This guide covers the most common causes of exercise-related shoulder pain, how to distinguish between them, and evidence-informed strategies for addressing each type.
Important: Persistent, severe, or worsening shoulder pain — or pain accompanied by weakness, numbness, or any trauma — should be evaluated by a licensed healthcare provider before any exercise modification is attempted.
The Most Common Causes of Exercise-Related Shoulder Pain
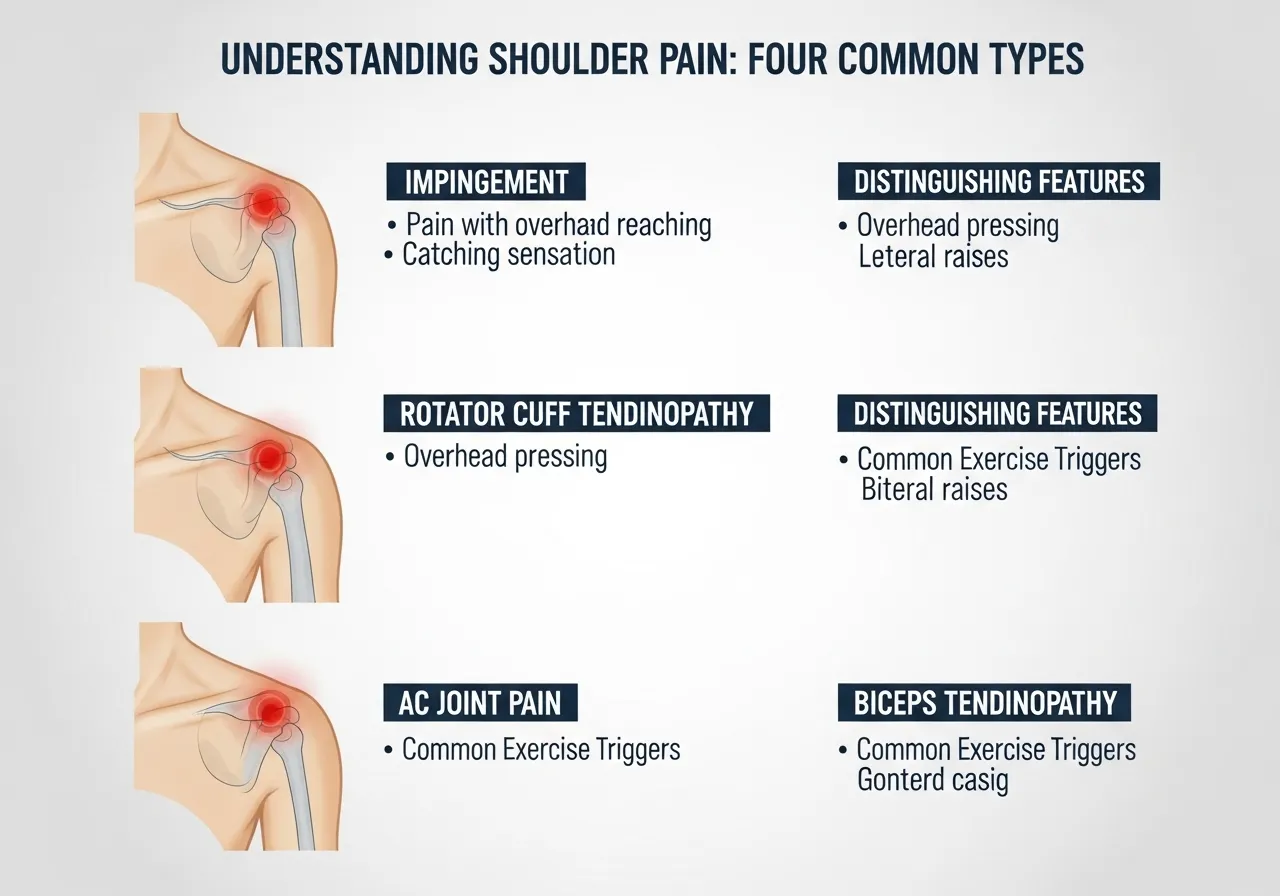
1 — Shoulder Impingement Syndrome
The most frequently encountered cause of shoulder pain in gym settings.
Impingement occurs when the soft tissue structures in the subacromial space (the narrow gap between the top of the humerus and the underside of the acromion bone) are compressed during arm elevation — producing a characteristic pinching pain, often felt between 60–120° of arm elevation.
Common exercise triggers: Overhead pressing, lateral raises, pull-ups, and upright rows — particularly with poor scapular mechanics or tight posterior capsule.
2 — Rotator Cuff Strain or Tendinopathy
The rotator cuff consists of four muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) that stabilize the glenohumeral joint and assist rotation.
Rotator cuff tendinopathy (a chronic overuse condition involving structural changes within the tendon without necessarily an acute tear) typically develops gradually from repetitive overhead loading or excessive pressing volume without adequate posterior chain balance.
Distinguishing feature: Pain with resisted external rotation (turning the arm outward against resistance) often implicates the posterior rotator cuff; pain with resisted internal rotation or overhead pressing suggests the subscapularis or supraspinatus.
3 — AC Joint Issues
The acromioclavicular (AC) joint (where the clavicle meets the acromion at the top of the shoulder) can become irritated from heavy pressing or direct impact.
Distinguishing feature: Pain at the very top of the shoulder, often worsened by cross-body movements (reaching across the chest) and heavy barbell pressing with very wide grip.
4 — Bicep Tendon Involvement
The long head of the biceps tendon runs through the shoulder joint and can become inflamed from repetitive overhead or curling movements.
Distinguishing feature: Pain at the front of the shoulder, in the bicipital groove (a groove in the humerus where the long head of the biceps tendon passes), often worsened by supinated curls and overhead pressing.
The Most Common Contributing Factors (and Why They Matter)
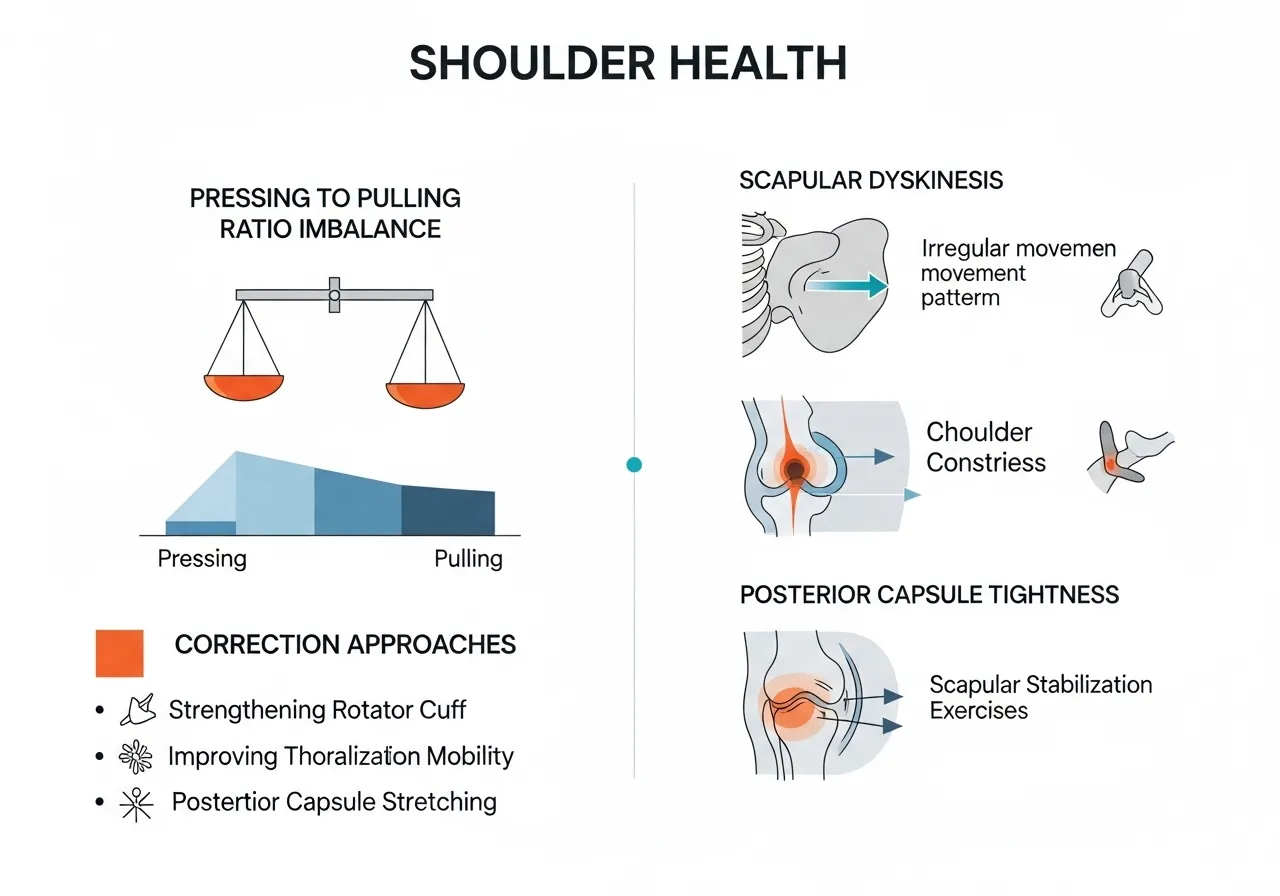
Pressing-to-Pulling Imbalance
The single most common structural contributor to exercise-related shoulder problems in gym athletes: performing significantly more pressing volume than pulling volume.
Pressing (bench press, overhead press, push-ups) develops the anterior deltoid and pectorals — muscles that internally rotate the shoulder.
Without adequate pulling volume (rows, face pulls, band pull-aparts), the posterior rotator cuff and scapular retractors become relatively weak, allowing the humeral head to migrate anteriorly (forward in the joint socket) — increasing impingement risk during arm elevation.
Practical guideline: Maintaining approximately a 1:1 ratio of horizontal pulling to horizontal pressing sets per week is a widely recommended starting point for shoulder health maintenance.
Poor Scapular Control
Scapular dyskinesis (abnormal movement patterns of the shoulder blade during arm elevation) is strongly associated with shoulder impingement in research literature.
The scapula should rotate upward as the arm rises — if it instead elevates (shrugs) or tips forward, the subacromial space narrows and compression of the rotator cuff tendons increases.
Tight Posterior Shoulder Capsule
A tight posterior shoulder capsule (the connective tissue at the back of the shoulder joint) forces the humeral head to migrate anteriorly and superiorly during arm elevation — a direct contributor to impingement.
The sleeper stretch (lying on the affected side and gently rotating the forearm downward toward the bed or floor) is the most commonly prescribed intervention for posterior capsule tightness.
Exercise Modifications for Common Shoulder Pain Patterns
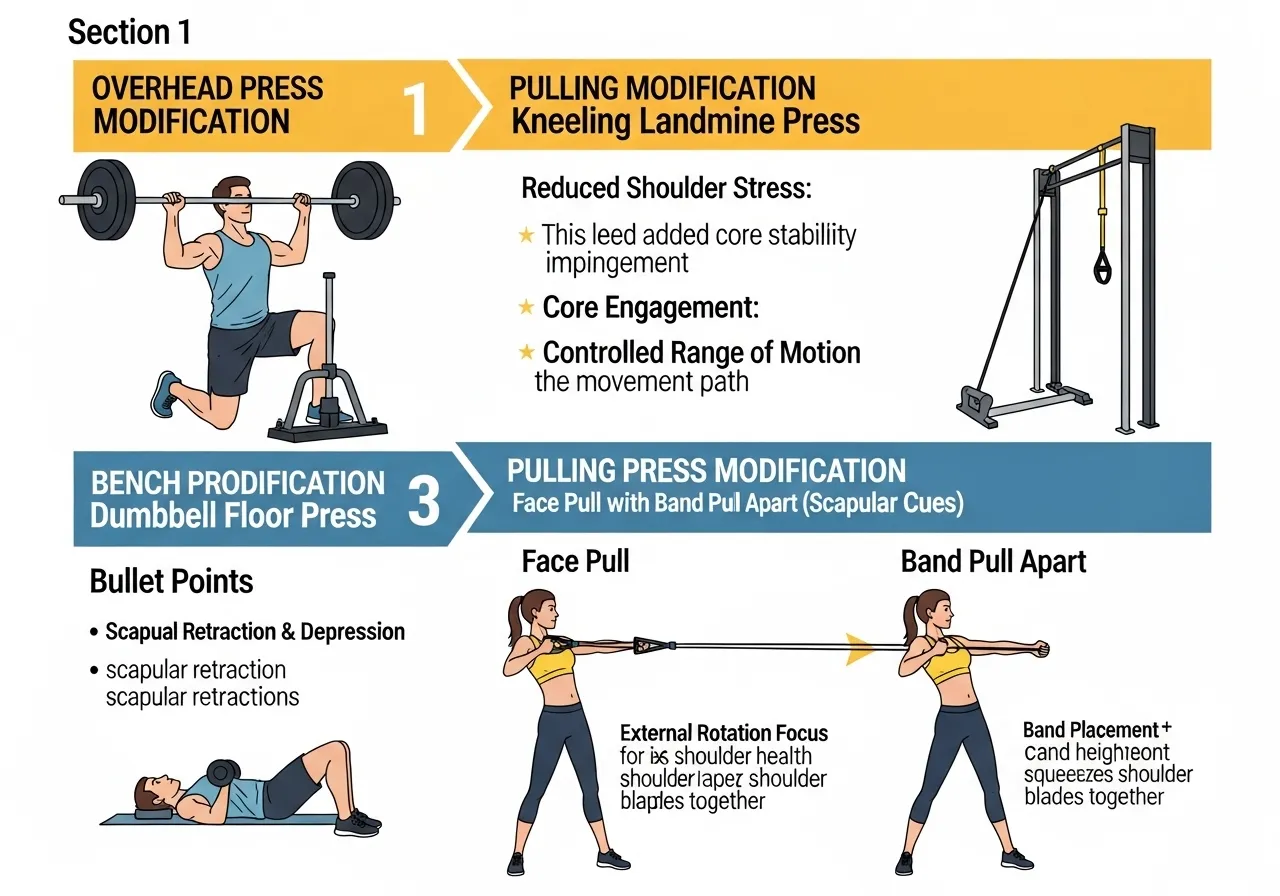
If Pain Occurs During Overhead Pressing
✅ Reduce range of motion temporarily — stopping 10–15° short of full overhead extension may reduce impingement
✅ Add face pulls (3 × 15–20) before every pressing session to pre-activate posterior rotator cuff
✅ Reduce pressing load and volume while symptoms are present
If Pain Occurs During Pulling Exercises
✅ Focus on initiating the pull with scapular depression before elbow flexion begins
✅ Avoid behind-the-neck pulling variations — these place the shoulder in a mechanically compromised position
If Pain Occurs During Bench Press
✅ Reduce elbow flare — maintaining 45–60° rather than 90° reduces AC joint and anterior capsule stress
✅ Use dumbbells temporarily — allows each arm to follow its natural joint path
A General Principle Worth Emphasizing
Exercise modification should be directed at identifying what can be trained without reproducing pain — not simply stopping all shoulder training.
Maintaining movement and loading in pain-free ranges typically supports better recovery outcomes than complete rest, according to current tendinopathy management guidelines.
Rehabilitation Exercises for Shoulder Health
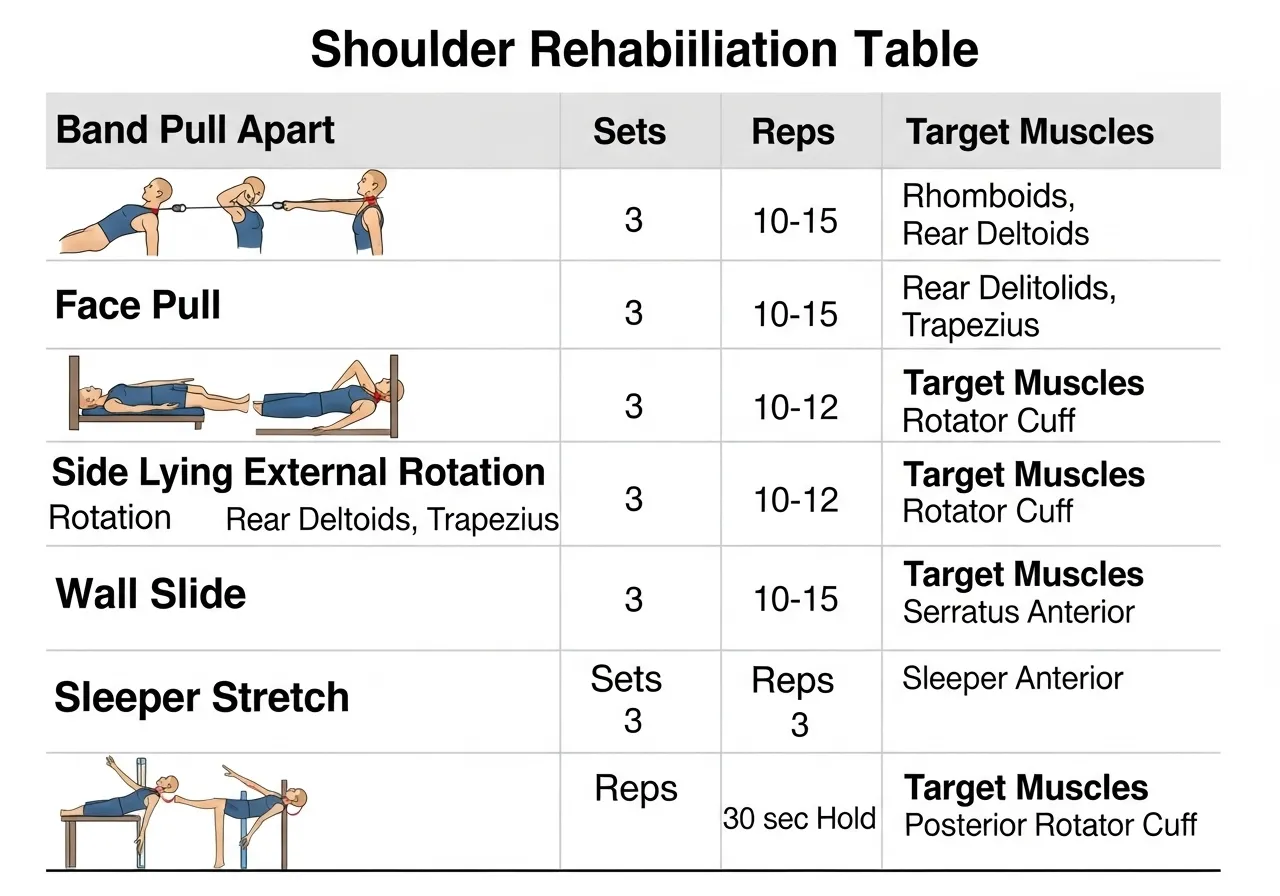
For Posterior Rotator Cuff and Scapular Stabilizers
| Exercise | Target | Suggested Sets × Reps |
|---|---|---|
| Band pull-apart | Posterior deltoid, rhomboids | 3 × 15–20 |
| Face pull (cable or band) | External rotators, rear deltoid | 3 × 15 |
| Side-lying external rotation | Infraspinatus, teres minor | 3 × 12–15 each side |
| Wall slide | Lower trapezius, serratus anterior | 3 × 10 |
| Sleeper stretch | Posterior shoulder capsule | 3 × 30 sec each side |
When to Seek Professional Evaluation
• Pain does not improve with 2–3 weeks of load modification and rehabilitation exercises
• Pain is present at rest or disturbs sleep
• Weakness is present — difficulty raising the arm or holding objects at shoulder height
• A specific incident (fall, impact, sudden force) preceded the pain
• Clicking, catching, or a sensation of the shoulder “giving way”

Frequently Asked Questions About Shoulder Pain and Exercise
Q: Can I keep training with shoulder pain?
In many cases, yes — with appropriate modification.
The key is identifying which specific movements reproduce the pain and temporarily replacing them with pain-free alternatives, while adding posterior chain rehabilitation work.
Continuing to train the same exercises at the same load through pain is unlikely to resolve the underlying issue and may worsen it. Complete cessation, on the other hand, may allow weakness and stiffness to develop that complicates recovery.
Pain that is sharp, neurological (numbness or tingling), or accompanied by significant weakness warrants professional evaluation before continuing training.
Q: Will impingement go away on its own?
Mild impingement symptoms often improve with load modification, posterior chain strengthening, and posterior capsule stretching — without requiring medical intervention.
Symptoms that persist beyond 4–6 weeks of conservative management, or that progressively worsen, warrant evaluation by a sports medicine physician or physical therapist, as imaging may be needed to assess whether structural involvement (rotator cuff tendon tear, labral issue) is present.
Q: Is it safe to resume overhead pressing after shoulder pain resolves?
Generally yes — with gradual reintroduction. Starting at lower loads than pre-injury, using dumbbell variations before returning to the barbell, and maintaining the posterior chain work that supported recovery are generally recommended approaches.
Rushing back to pre-injury loads before the underlying factors have been addressed is a common cause of recurrence.
- Pressing-to-pulling imbalance is the most common structural contributor to gym-related shoulder problems
- Face pulls, band pull-aparts, and external rotation exercises are foundational shoulder health maintenance tools
- Exercise modification (finding pain-free alternatives) is generally preferable to complete training cessation
- Posterior capsule tightness and poor scapular control are frequently addressable causes of impingement
- Seek professional evaluation for pain that is severe, worsening, neurological, or persists beyond 4–6 weeks





