
What Is DOMS and How Do You Deal With It?
⚠️ Disclaimer: The information in this article is for general educational purposes only and does not constitute medical, nutritional, or professional fitness advice. Individual results may vary. Always consult a qualified healthcare professional or certified fitness trainer before starting any new exercise program, changing your diet, or making decisions about injury treatment or recovery. If you experience pain, discomfort, or any unusual symptoms during exercise, stop immediately and seek professional guidance.

What Is DOMS? The Science of Delayed Onset Muscle Soreness Explained
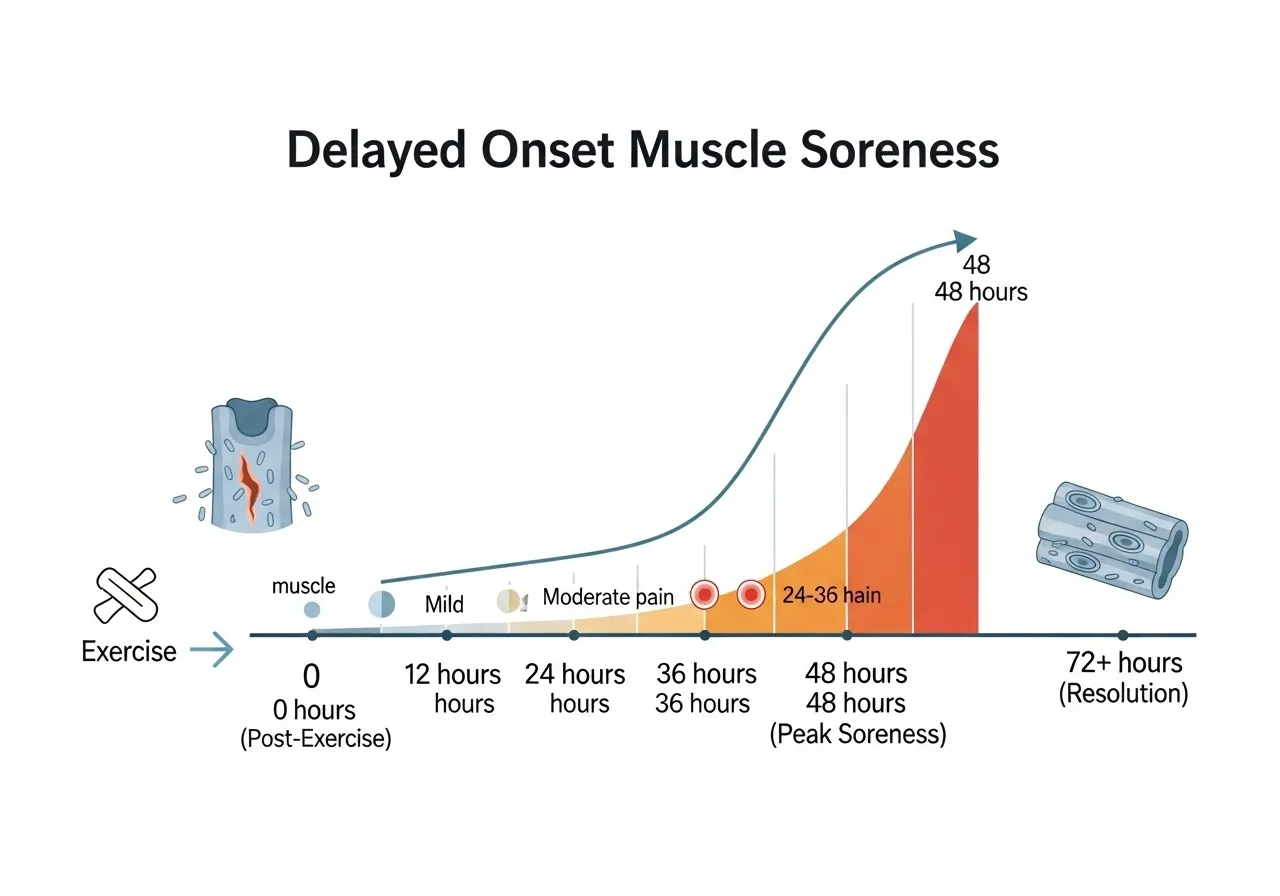
Delayed onset muscle soreness — the stiffness, tenderness, and sometimes dramatic pain that appears 24–72 hours after unfamiliar or intense exercise — is one of the most universally experienced and most misunderstood phenomena in physical training. The experience is familiar to virtually every person who has ever started a new exercise program, returned to training after a break, or dramatically increased training volume: the workout feels manageable, the day after feels fine, and then day two arrives with the kind of muscle soreness that makes walking downstairs a deliberate, wincing process. Understanding what DOMS actually is — and what it is not — is the foundation for managing it effectively rather than either ignoring it inappropriately or catastrophizing it into training paralysis.
Defining DOMS: Symptoms and Timeline
DOMS is characterized by a specific cluster of symptoms that distinguish it from acute muscle pain (which occurs during exercise) and from injury (which typically presents differently): muscular tenderness to touch (pressing on the affected muscle hurts), stiffness and reduced range of motion (the muscle feels tight and resists stretching), reduced strength (temporary strength loss of 20–50% has been measured in significantly DOMS-affected muscles), and swelling in the affected area (particularly after eccentric-heavy exercise like downhill running or heavy squatting with new training volumes). The critical temporal feature of DOMS — and the source of the “delayed onset” designation — is that symptoms peak 24–72 hours after the causative exercise rather than immediately following it. The workout itself typically feels fine; the soreness arrives the next day or the day after, peaks at 48 hours in most cases, and gradually resolves over 3–5 days without treatment.
DOMS vs. Injury: The Critical Distinction
The most practically important understanding of DOMS is its distinction from muscle injury — the difference between the normal physiological response to novel exercise stress that indicates adaptation is occurring, and the abnormal tissue damage that indicates something is actually wrong. DOMS characteristics: bilateral symmetry (both legs are equally sore after squatting), affects muscles that were specifically exercised, resolves progressively over 3–5 days without worsening, does not cause acute sharp pain during exercise (only soreness during and after stretching), and typically presents with familiar muscle belly tenderness rather than joint pain or specific pain points. Injury characteristics: typically unilateral or asymmetric, may include acute sharp pain during exercise, may worsen rather than improve over 48–72 hours, and often presents with specific pain points at muscle-tendon junctions or joints rather than diffuse muscle belly tenderness. When in doubt: DOMS that does not progressively improve after 5–7 days, that is associated with significant swelling and warmth suggesting inflammatory response beyond normal, or that includes severe strength loss that does not begin recovering at 48 hours should prompt professional evaluation to rule out muscle tear or rhabdomyolysis (the serious condition of massive muscle breakdown that requires medical attention).
Who Gets DOMS and When
DOMS is not exclusively a beginner phenomenon, though beginners experience it most severely and most frequently. Any athlete — regardless of training age — can experience DOMS when performing movements that are novel to their training history, performing familiar movements at dramatically higher volumes than usual, or returning to training after a period of detraining. The repeated bout effect — the phenomenon where the same exercise produces progressively less soreness with each repetition — means that experienced athletes are protected from DOMS specifically in the movements they train regularly, while remaining vulnerable to it in any exercise that falls outside their established movement repertoire. Research published in the British Journal of Sports Medicine on repeated bout effect and DOMS consistently finds that 2–3 exposures to any given novel exercise dramatically reduces subsequent DOMS from that exercise — suggesting that strategic program design can minimize DOMS without sacrificing training novelty.
DOMS Is Not a Requirement for Muscle Growth
The persistent belief that soreness confirms effective training — “no pain, no gain” in its specific DOMS manifestation — is one of the most consequential fitness myths to debunk, because it leads athletes to pursue soreness as a proxy for progress rather than tracking actual performance improvements. DOMS indicates muscle stress from novel exercise stimulus — it does not reliably indicate that hypertrophy or strength adaptation will result, and its absence does not indicate that adaptation is not occurring. Well-trained athletes who rarely experience DOMS continue to make strength and hypertrophy gains from training that produces no soreness because their muscles have adapted to the training stimulus they regularly experience. Soreness is a consequence of exercise novelty and the specific inflammatory and microtrauma responses that follow it — not a prerequisite for adaptation. Chasing soreness by constantly varying exercises and dramatically increasing loads produces chronic, recurring DOMS that impairs performance and recovery more than it contributes to adaptation. Progressive overload on consistent movements — gradually increasing the load or volume of the exercises that reliably produce adaptation — produces superior long-term results with far less debilitating soreness than the constantly varied, soreness-maximizing approach.
DOMS in Different Training Contexts
The practical experience of DOMS varies significantly across training contexts, affecting how it should be managed. Beginners starting a resistance training program: typically experience significant DOMS in the first 2–4 weeks of training as the body adapts to a completely novel stress — this initial DOMS is normal, expected, and self-limiting as the repeated bout effect reduces it across subsequent weeks. Athletes returning from injury layoffs: frequently experience significant DOMS when resuming training because the detraining period has reversed the repeated bout effect protection — the muscles respond to resumed training with a fresh first-exposure soreness that requires managed progression to prevent excessive impairment. Athletes introducing new movements or dramatically increasing volume: experience DOMS specific to the novel stimulus while maintaining normal function in well-established movements — managed by progressive introduction of new exercises rather than attempting maximum volume immediately. Understanding which of these contexts applies to current training allows appropriately calibrated management expectations and prevents the panic response to significant DOMS that leads athletes to stop training just as the adaptation process is beginning.
Rhabdomyolysis: When DOMS Becomes a Medical Emergency
At the extreme end of exercise-induced muscle damage lies rhabdomyolysis — the catastrophic breakdown of muscle tissue that releases myoglobin into the bloodstream, overwhelming the kidneys’ filtration capacity and potentially causing acute kidney failure. While true rhabdomyolysis is far rarer than typical DOMS, the exercise contexts that most frequently produce it have become more common: CrossFit-style high-intensity workouts with extremely high volumes of eccentric exercise in unconditioned individuals, spinning classes for complete beginners, and extreme exercise challenges undertaken without progressive conditioning. The distinguishing features of rhabdomyolysis versus severe DOMS: cola-colored or dark brown urine (myoglobin in the urine), severe swelling in the affected muscles, muscle pain that is dramatically disproportionate to the exercise performed, nausea and vomiting, confusion or unusual fatigue, and reduced or absent urine output — any combination of these signs following intense exercise requires immediate medical evaluation. Treatment requires intravenous fluid therapy to protect kidney function and may require hospitalization. The prevention message: progressive training load increases and appropriate conditioning before high-volume eccentric exercise events are not optional precautions but safety requirements — the athlete who goes from no exercise to maximum-intensity boutique fitness class is genuinely at medical risk, not just uncomfortable.
DOMS and Athletic Performance: The Functional Impact
The performance implications of significant DOMS extend beyond the subjective discomfort — objective strength, power, and movement quality are measurably impaired during the DOMS period in ways that affect both training quality and injury risk. Research on strength during DOMS consistently finds 20–50% reductions in maximal voluntary contraction in severely DOMS-affected muscles at 24–48 hours post-exercise — meaning that a training session performed during peak DOMS produces significantly lower training stimulus than the same session performed on non-DOMS muscle. The injury risk dimension: DOMS-induced altered proprioception and reduced force production impairs the neuromuscular control of movement, increasing the risk of compensatory patterns during loaded exercises that place unusual stress on joints and connective tissue. Understanding this performance impairment argues for adjusting training intensity and technique demands when significant DOMS is present — reducing loads, avoiding maximum effort sets on affected muscles, and prioritizing non-affected muscle groups — rather than training through DOMS as if it were not a physiological reality affecting performance safety and quality.
DOMS Research: What the Evidence Actually Shows
The scientific literature on DOMS is extensive, with hundreds of studies investigating its mechanisms, recovery interventions, and prevention strategies — and the accumulated evidence has overturned several popular beliefs about what DOMS is and how it should be managed. The research from the American College of Sports Medicine on exercise-induced muscle damage establishes that the primary DOMS mechanism is not lactic acid accumulation (as was believed for decades and is still commonly repeated) but eccentric exercise-induced microstructural muscle damage — specifically, disruption of the Z-disk structure of sarcomeres during forceful eccentric loading. The immune-mediated inflammatory cascade that follows this microstructural damage — involving neutrophil infiltration, cytokine release, prostaglandin production, and eventually macrophage-mediated tissue repair — is what produces the pain, swelling, and functional impairment characteristics of DOMS. This mechanistic understanding guides the effective interventions: treatments that reduce the inflammatory cascade (anti-inflammatories, cold therapy) provide symptomatic relief but may interfere with the adaptation process; treatments that support recovery without suppressing adaptation (adequate protein, sleep, light movement) produce optimal outcomes for both comfort and long-term training adaptation.
The physiological framework of DOMS — its mechanisms, timeline, performance implications, and distinction from injury — provides the foundation for the evidence-based management strategies in the sections that follow. Understanding why DOMS occurs as a normal adaptive response to novel exercise, rather than a sign of damage or inadequate recovery, removes the anxiety that often accompanies significant soreness and replaces it with the informed confidence to manage it appropriately. Understanding DOMS completely — its mechanisms, timeline, functional consequences, and the distinction from injury — converts soreness from a source of training anxiety into a manageable, interpretable physiological signal that informs training decisions rather than disrupting them. The athlete who understands DOMS at the mechanistic, strategic, and psychological level described in this article trains with the informed confidence that converts soreness from a barrier to consistent training into a familiar, manageable signal of productive adaptation — the mark of the evidence-informed, resilient athletic practice that produces long-term fitness results independent of the inevitable discomforts that progressive training always involves. DOMS research has evolved significantly in the past two decades — moving from the discredited lactic acid hypothesis through connective tissue damage theories to the current consensus on eccentric-induced sarcomere disruption and inflammatory cascade — and the practical management strategies derived from this improved mechanistic understanding are dramatically more effective than the approaches based on outdated theories that still dominate much popular fitness advice. The comprehensive DOMS guide in this article — from the physiological mechanisms through the evidence-based recovery strategies, prevention protocols, myth debunking, and personalized management framework — provides every tool an athlete needs to transform their relationship with soreness from anxious avoidance or uninformed endurance into the intelligent, evidence-based management practice that makes DOMS a temporary, manageable component of productive athletic training rather than a recurring barrier to training consistency and performance.

What Causes DOMS: Mechanisms, Risk Factors, and the Eccentric Exercise Connection
Understanding what causes DOMS — not just “intense exercise” in the generic sense, but the specific exercise characteristics and physiological mechanisms that produce the soreness — allows athletes to predict when DOMS will occur, understand why certain exercises cause it more reliably than others, and design training intelligently around the DOMS risk that specific exercise types carry. The primary mechanism is well-established: eccentric muscle contractions, combined with exercise novelty, produce the microstructural damage that initiates the inflammatory cascade underlying DOMS. But the specific features of eccentric loading, exercise novelty, and individual variation that determine DOMS severity are worth understanding in detail.
Eccentric Exercise: The Primary DOMS Driver
Eccentric muscle contractions — those in which the muscle produces force while lengthening — produce dramatically more DOMS than concentric contractions (shortening under load) or isometric contractions (static force production without movement). The reason: during eccentric loading, fewer motor units are recruited to produce a given force level compared to concentric loading (because the eccentric mechanism is inherently more mechanically efficient at producing force), meaning each active muscle fiber bears greater mechanical stress per unit of effort. This higher mechanical stress per fiber produces greater disruption of the sarcomere structure — the Z-disks that anchor the contractile proteins within the sarcomere are physically deformed by the high eccentric forces, producing the microstructural damage that initiates the inflammatory repair process. The exercises most reliably associated with significant DOMS are those with prominent eccentric loading phases: the lowering phase of squats, the eccentric lowering of a pull-up or chin-up, downhill running (quadriceps eccentrically control descent against gravity), Nordic hamstring curls (high eccentric hamstring loading), and the lowering phase of plyometric exercises. Exercises with primarily concentric loading — cycling, rowing machine (when performed without emphasis on the recovery phase), and concentric-only training protocols — produce significantly less DOMS at equivalent effort levels.
Exercise Novelty: Why DOMS Decreases With Repetition
Exercise novelty is the second primary DOMS determinant — familiar exercises produce dramatically less soreness than novel ones regardless of the absolute intensity applied. The repeated bout effect explains this: the first exposure to any exercise produces the greatest DOMS because the neuromuscular, metabolic, and structural adaptations that reduce susceptibility have not yet occurred. By the second exposure to the same exercise (even weeks later), DOMS is typically reduced by 50–75%; by the third to fourth exposure, the exercise produces minimal soreness. The proposed mechanisms of the repeated bout effect include: increased motor unit recruitment efficiency (more even distribution of force across more motor units, reducing per-fiber mechanical stress), improved sarcomere mechanical stability (structural adaptation in the Z-disk region that increases resistance to eccentric-induced damage), altered muscle architecture (shift to longer optimal fiber length that reduces mechanical vulnerability), and enhanced protein synthesis response (faster initiation of repair processes that limit cumulative damage). This rapid adaptation means that DOMS is a physiologically necessary but transient response — the first few exposures to any new exercise involve DOMS as an adaptation cost, and subsequent exposures are paid progressively less soreness as the protective adaptations establish.
Individual Risk Factors for Severe DOMS
Several individual characteristics influence DOMS severity beyond exercise type and novelty, explaining why two athletes performing identical workouts experience dramatically different soreness levels. Training age and fitness level: paradoxically, moderate fitness level (enough conditioning to perform higher training volumes) combined with low exercise-specific conditioning (unfamiliar with the specific movement) produces worse DOMS than either very low fitness (cannot perform sufficient volume to cause significant damage) or very high fitness (has accumulated repeated bout protection). This explains why recreational athletes joining a CrossFit gym often experience more severe DOMS than complete beginners doing the same class at lower intensity. Sex and hormonal environment: research on sex differences in DOMS finds inconsistent results, but some evidence suggests estrogen may have mild muscle-protective effects that reduce eccentric damage in women — though this does not translate to clinically meaningful differences in management approaches. Genetics: individual variation in inflammatory response genes (including variants in cytokine production pathways) contributes to DOMS severity differences that cannot be explained by training or lifestyle factors — some people are simply more DOMS-prone than others regardless of conditioning level. Body composition: higher lean mass relative to body weight is associated with greater eccentric force production capacity and therefore potentially greater per-session eccentric loading — strong, muscular athletes may actually experience more severe DOMS from genuinely intense eccentric sessions than less muscular individuals performing the same relative intensity.
The Inflammatory Cascade: From Microtrauma to Soreness
The timeline between the causative exercise and peak DOMS symptoms (24–72 hours) reflects the physiological process of the inflammatory cascade that converts exercise-induced microstructural damage into the pain, swelling, and functional impairment that characterize DOMS. Immediately after exercise: structural damage to sarcomeres (Z-disk disruption) occurs; mechanical disruption of cell membranes allows calcium to enter muscle cells, triggering further protein degradation. Hours 2–6: neutrophil infiltration into the damaged muscle tissue begins — the first immune cell responders that initiate inflammation to clear debris and signal the repair response. Hours 6–24: increased prostaglandin production sensitizes pain receptors (nociceptors) in the muscle — this peripheral sensitization, not direct nerve damage, produces the tenderness to touch that characterizes DOMS. Hours 24–72: macrophage infiltration and peak inflammatory cytokine levels coincide with peak DOMS symptoms; protein synthesis begins to increase as satellite cell activation initiates the muscle repair and remodeling process. Days 3–5: inflammatory response resolves, repair processes conclude, and DOMS symptoms progressively diminish. Research on this cascade mechanism published in the PubMed DOMS literature has guided the development of recovery interventions that target specific steps in this process.
Exercise Types Ranked by DOMS Risk
Understanding which exercises carry the highest DOMS risk allows strategic training design that manages soreness exposure relative to training goals. Highest DOMS risk (novel, high-volume eccentric): downhill running, Nordic hamstring curls, heavy squats and deadlifts with new training populations, plyo-focused training (jump squats, box jumps), and any exercise performed for the first time at high volume. High DOMS risk (familiar but volume-sensitive eccentric): pull-ups and rows at high volumes for those with moderate upper body strength, weighted lunges and step-downs, bench press with heavy eccentric emphasis. Moderate DOMS risk (concentric-dominant with eccentric component): standard barbell squats and deadlifts at training-adapted volumes, overhead pressing, and most standard gym exercises performed within established volume ranges. Low DOMS risk (primarily concentric or isometric): cycling, swimming, rowing machine, elliptical trainer at moderate intensity, and isometric training modalities that avoid high eccentric loading. This risk hierarchy guides the progressive introduction of high-DOMS-risk exercises, particularly for athletes returning from injury or beginning new training modalities.
Age and DOMS: How Soreness Changes With Aging
The relationship between aging and DOMS is multifaceted — older adults experience DOMS differently from younger athletes in ways that affect both management and training design. Research on aging and exercise-induced muscle damage finds that older adults (50+) may experience similar or greater levels of DOMS following novel eccentric exercise compared to younger adults, with potentially slower recovery timelines. The mechanisms contributing to age-related DOMS differences: reduced satellite cell density and activity (slower muscle repair response), decreased anti-inflammatory capacity (slower resolution of the inflammatory cascade), reduced protein synthesis rate (slower structural repair), and potentially altered pain perception. The practical implication for older athletes: more conservative progressive volume increases are appropriate when introducing novel eccentric exercises, with longer rest periods between high-DOMS-risk sessions to allow the additional time the recovery process requires. The good news: the repeated bout effect operates identically in older adults — the protective adaptations from repeated exposure reduce subsequent DOMS as reliably in older athletes as younger ones, and the long-term tissue conditioning from consistent training diminishes DOMS susceptibility across age groups regardless of the absolute recovery rate difference from acute bouts.
DOMS in Specific Sports: Runner’s DOMS, Lifter’s DOMS, and Swimmer’s DOMS
Sport-specific DOMS patterns reflect the eccentric loading profile of each sport’s movement demands. Runners experience DOMS most severely in the quadriceps and calves after downhill running or longer races — the quadriceps’ eccentric control of knee flexion during downhill running is particularly potent at producing DOMS in athletes who have not specifically conditioned for the downhill eccentric demand. Many experienced flat-course runners who never experience DOMS from their regular training develop significant soreness from their first mountain race or trail run with significant descent. Lifters experience DOMS patterns that reflect their specific exercise selection — a powerlifter primarily focused on high-bar squat will have conditioned for that specific movement’s eccentric demand but may experience significant DOMS when switching to Romanian deadlifts that load the hamstrings eccentrically in a different pattern. Swimmers rarely experience the classical muscle belly DOMS of land-based training because swimming’s buoyancy largely eliminates the eccentric loading component of movement — the muscles shorten against resistance (concentric) but rarely lengthen under high load in the eccentric pattern that produces DOMS. This is why swimmers who begin strength training commonly report dramatic DOMS from their first sessions — their muscles lack the repeated bout protection for land-based eccentric loading despite excellent swimming-specific conditioning.
Nutritional Factors That Influence DOMS Susceptibility
Several nutritional factors modulate DOMS severity through their effects on the inflammatory cascade, muscle repair processes, and antioxidant defense systems that determine how severely exercise-induced microtrauma progresses to clinical DOMS. Omega-3 fatty acids: EPA and DHA have anti-inflammatory properties that reduce the prostaglandin production responsible for DOMS pain sensitization — research finds that omega-3 supplementation (2–4g EPA+DHA daily) reduces DOMS severity and duration, with effects most pronounced after 4–8 weeks of supplementation that allows tissue omega-3 levels to fully elevate. Vitamin D: sufficient vitamin D status (blood 25-OH-D above 40–60 nmol/L) is associated with reduced exercise-induced muscle damage markers and faster recovery — the large proportion of athletes with vitamin D insufficiency may have greater DOMS susceptibility from this mechanism. Protein intake: adequate protein (2.0g/kg daily) provides the amino acid availability that supports the rapid initiation of muscle repair following eccentric damage — protein-deficient athletes show slower recovery from exercise-induced muscle damage than those meeting protein targets. These nutritional factors do not eliminate DOMS but represent the chronic dietary foundation that determines baseline DOMS susceptibility before any specific acute intervention is applied.
The mechanistic understanding of DOMS — eccentric loading as the primary driver, exercise novelty as the amplifying factor, and the inflammatory cascade as the physiological process — provides the rational foundation for every recovery and prevention strategy that follows, converting DOMS management from intuitive guesswork into evidence-based physiological intervention. The eccentric loading mechanism, exercise novelty effect, and individual risk factors that determine DOMS severity provide the predictive framework that allows athletes to anticipate when significant soreness will occur and prepare their training schedule and recovery protocols accordingly. The athlete who understands DOMS at the mechanistic, strategic, and psychological level described in this article trains with the informed confidence that converts soreness from a barrier to consistent training into a familiar, manageable signal of productive adaptation — the mark of the evidence-informed, resilient athletic practice that produces long-term fitness results independent of the inevitable discomforts that progressive training always involves. The sport-specific and population-specific DOMS patterns — the quadriceps-dominant soreness of new runners, the hamstring DOMS of Nordic curl initiates, the age-related slower resolution of older athletes — allow individualized prevention and management approaches that generic advice cannot provide, making this mechanistic knowledge practically valuable beyond its intellectual interest. The comprehensive DOMS guide in this article — from the physiological mechanisms through the evidence-based recovery strategies, prevention protocols, myth debunking, and personalized management framework — provides every tool an athlete needs to transform their relationship with soreness from anxious avoidance or uninformed endurance into the intelligent, evidence-based management practice that makes DOMS a temporary, manageable component of productive athletic training rather than a recurring barrier to training consistency and performance.
How to Recover From DOMS: Evidence-Based Strategies That Actually Work
The DOMS recovery intervention landscape is crowded with conflicting claims, placebo-dependent traditions, and genuinely evidence-supported strategies that are difficult to distinguish without examining the research quality. This section separates the interventions with consistent research support from those with weak or no evidence, providing the practical recovery toolkit that makes DOMS periods more manageable without wasting time and money on ineffective approaches.
Active Recovery: The Best Evidence-Based DOMS Strategy
Active recovery — low-intensity movement of the affected muscles at 20–40% of maximum effort — is the most consistently supported DOMS recovery intervention in the research literature, producing reliable reductions in DOMS severity and duration compared to complete rest. The mechanism: low-intensity muscle contractions increase local blood flow, accelerating the removal of inflammatory mediators, delivering nutrients for repair, and reducing the edema (fluid accumulation) that contributes to the pressure-related pain of DOMS. Research consistently finds that 20–30 minutes of easy cycling, walking, swimming, or any light movement involving the DOMS-affected muscles produces meaningful pain reduction for 4–6 hours following the session — not permanent resolution, but sufficient relief to allow normal function and productive light training. Active recovery does not require the affected muscles to be the primary focus: a 30-minute easy walk after quad-dominant DOMS increases lower extremity blood flow and reduces soreness even though the walk is a lower-intensity stimulus for the same muscles. The practical implementation: on days following high-DOMS-risk training sessions, schedule 20–30 minutes of easy movement rather than complete rest — a Zone 1 bike ride, a 20-minute easy walk, light yoga, or a casual swim all qualify. The NSCA’s evidence-based recovery guidelines for athletes list active recovery as the highest-evidence intervention for DOMS management across the research literature.
Ice Baths and Cold Water Immersion
Cold water immersion (CWI) — immersing the body or affected limbs in cold water at 10–15°C for 10–15 minutes post-exercise — is among the most researched DOMS interventions and produces consistent reductions in perceived soreness and functional impairment in the 24–72 hour post-exercise period. The mechanism: cold-induced vasoconstriction reduces the inflammatory cascade’s progression by limiting prostaglandin production, reducing edema formation, and slowing the metabolic processes of the inflammatory response. Research from the Journal of Strength and Conditioning Research on cold water immersion and DOMS finds consistent 20–40% reductions in perceived soreness at 24 and 48 hours post-exercise compared to passive rest. The important caveat: the same anti-inflammatory mechanism that reduces DOMS may also blunt the adaptation signal that triggers the muscle remodeling and strength gains that training is designed to produce. Research on cold water immersion and long-term adaptation finds that regular post-training CWI reduces hypertrophy and strength gains over 12-week training periods compared to passive recovery — suggesting that CWI is most appropriate when minimizing soreness for competition or performance maintenance is the priority, and less appropriate during hypertrophy or strength development phases where maximizing adaptation is the goal. Protocol: 10–15 minutes at 10–15°C (cold but not painfully so), immediately post-exercise or within 1 hour, with the affected body region submerged. Cold showers are a practical alternative that produces milder but real benefits at lower barrier.
Massage and Foam Rolling
Massage therapy for DOMS — whether from a therapist or via self-administered foam rolling — provides meaningful subjective pain relief through mechanisms that include increased local circulation, mechanical disruption of pain-sensitized tissue, and the neurological effects of tactile stimulation on pain perception. Research on massage timing for DOMS finds that massage administered 24–48 hours post-exercise (at peak soreness) produces the most consistent pain reduction — with effects persisting for several hours following the session. Foam rolling as a self-massage substitute: research on foam rolling for DOMS consistently finds reductions in perceived soreness and improvements in range of motion, with smaller effect sizes than professional massage but with the practical advantages of daily availability, zero cost after initial equipment purchase, and controllable pressure. Foam rolling protocol for DOMS: 60–90 seconds of slow rolling per muscle group with pauses on tender spots, performed either before training sessions (improves range of motion) or as a dedicated recovery session (reduces soreness for several hours). The mechanism of foam rolling’s DOMS reduction is debated — proposed mechanisms include fascial hydration changes, neural pain modulation, and the same circulation benefits of active recovery. Regardless of mechanism, the consistent research finding is that foam rolling reduces perceived soreness without the adaptation-blunting risk of cold water immersion, making it a preferable daily recovery tool for athletes in active training phases.
Nutrition for DOMS Recovery: What Helps, What Doesn’t
Several nutritional interventions with research support for DOMS recovery provide practical additions to the physical recovery toolkit. Tart cherry juice: the most research-supported nutritional DOMS intervention, with multiple randomized controlled trials finding that 240ml of tart cherry juice (or 30ml concentrate) consumed twice daily — beginning 4–5 days before a high-DOMS-risk event and continuing for 2–3 days after — reduces DOMS severity by 20–30% compared to placebo. The mechanism: tart cherry’s anthocyanins and other polyphenols reduce inflammatory cytokine production and oxidative stress that contribute to DOMS. Protein intake: consuming 30–40g of high-quality protein (whey, eggs, Greek yogurt) within 60 minutes post-exercise initiates the muscle protein synthesis that begins the repair process — evidence does not show that this reduces DOMS perception, but it accelerates the structural recovery that resolves DOMS’s underlying cause. Creatine monohydrate: research on creatine and DOMS finds modest reductions in muscle damage markers and soreness with chronic loading (5g daily for 4+ weeks) — the mechanism likely involves creatine’s role in ATP resynthesis supporting the energy-intensive repair processes following eccentric damage. NSAIDs (ibuprofen, naproxen): reduce DOMS pain reliably through prostaglandin inhibition but carry the same adaptation-blunting concern as cold water immersion — routine NSAID use after training may impair muscle hypertrophy and strength adaptation with chronic use. Appropriate for occasional use when DOMS is functionally limiting, but not as a routine post-training intervention during active strength development phases.
Sleep: The Underrated DOMS Recovery Tool
Sleep is the most powerful DOMS recovery accelerator available because it is during sleep — particularly slow-wave sleep — that growth hormone secretion peaks, muscle protein synthesis rates are highest, and the immune-mediated repair processes that resolve DOMS operate at maximum efficiency. Research on sleep deprivation and muscle recovery consistently finds that insufficient sleep (below 7 hours) significantly impairs both the subjective resolution of DOMS and the objective recovery of muscle function — suggesting that strategic sleep optimization during DOMS periods accelerates recovery more than any specific active intervention. The practical sleep optimization for DOMS recovery: ensure 8–9 hours of sleep opportunity on the nights following high-DOMS-risk training sessions, particularly the first two nights when the inflammatory cascade is most active. Prioritizing sleep over other recovery modalities — when forced to choose between a 20-minute foam rolling session and 20 additional minutes of sleep — favors sleep for DOMS recovery, because the growth hormone and protein synthesis advantages of additional sleep time exceed the local circulation benefits of the foam rolling session.
Contrast Therapy: Alternating Hot and Cold
Contrast therapy — alternating between hot (38–40°C) and cold (10–15°C) water immersion or shower — produces DOMS relief through the repeated vasodilation and vasoconstriction cycle that creates a pumping effect on local blood flow, accelerating the removal of inflammatory mediators and edema. Research on contrast therapy for DOMS finds moderate evidence for reduced soreness at 24 and 48 hours compared to passive rest, with effect sizes similar to cold water immersion alone but without the strong adaptation-blunting evidence associated with isolated cold therapy. Practical contrast protocol: 3–4 cycles of 2 minutes hot / 1 minute cold, ending on cold, using either a contrast shower (alternating hot and cold water) or alternating submersion in hot and cold water containers. The reduced adaptation-blunting concern relative to CWI-only protocols and the practical accessibility of contrast showers makes this an appropriate routine recovery tool for training phases where both soreness management and adaptation preservation are priorities.
Compression Garments and DOMS
Compression garments — tight-fitting sleeves, tights, or socks that apply graduated pressure to muscle groups — have a growing evidence base for DOMS reduction through their effect on venous return, edema prevention, and proprioceptive feedback. Research on compression garments worn during and after eccentric exercise finds modest but consistent reductions in DOMS severity at 24–48 hours, reduced swelling, and faster recovery of muscle function compared to no compression. The mechanism: external compression reduces the fluid accumulation (edema) that contributes to the pressure-related pain component of DOMS, while improving venous return that accelerates the clearance of inflammatory mediators. Protocol: wear compression garments during training sessions with high DOMS risk and continue wearing for 12–24 hours post-exercise for maximum effect. The modest effect size means compression garments are most valuable as one component of a comprehensive recovery strategy rather than a standalone DOMS solution, but their practical accessibility, absence of adaptation-blunting risk, and comfort make them a worthwhile addition to the recovery toolkit for athletes who train with high DOMS risk regularly.
Combining Recovery Strategies: The Optimal DOMS Recovery Protocol
The most effective DOMS recovery approach combines multiple evidence-supported strategies whose mechanisms complement rather than duplicate each other. The optimal 48-hour DOMS recovery protocol: immediately post-exercise — 20–30 minutes of easy active recovery (light cycling or walking), followed by a cold shower or contrast therapy (3 rounds alternating hot/cold). Hours 2–6: consume 30–40g protein with tart cherry juice (240ml) if available. 24 hours post: 20–30 minute foam rolling session on affected muscles, maintain protein intake at 2.0g/kg daily, prioritize 8–9 hours sleep. 48 hours post: light active recovery session (easy yoga, walking, or swimming), second foam rolling session, continue adequate protein and tart cherry juice if using. This combined protocol addresses multiple mechanisms simultaneously — circulation (active recovery, contrast therapy), inflammation (tart cherry, adequate sleep), structural repair (protein intake, sleep), and pain perception (foam rolling, compression). The combined approach consistently outperforms any single intervention in comparative research, producing the fastest functional recovery and return to full training capacity.
The evidence hierarchy for DOMS recovery is clear: active recovery and adequate sleep are the highest-impact, zero-cost interventions available; cold therapy and foam rolling provide meaningful additional relief; nutritional supports like tart cherry juice and protein optimize the biochemical recovery environment. Together they constitute the comprehensive recovery toolkit that minimizes DOMS duration while preserving the training adaptations that the exercise was designed to produce. The evidence-based recovery toolkit — active recovery, cold therapy, foam rolling, tart cherry juice, protein, and sleep — addresses DOMS through multiple complementary mechanisms that together produce faster, more complete recovery than any single intervention alone. The athlete who understands DOMS at the mechanistic, strategic, and psychological level described in this article trains with the informed confidence that converts soreness from a barrier to consistent training into a familiar, manageable signal of productive adaptation — the mark of the evidence-informed, resilient athletic practice that produces long-term fitness results independent of the inevitable discomforts that progressive training always involves. Athletes who establish consistent recovery habits — the post-training foam rolling session, the tart cherry juice protocol before high-risk training events, the prioritized sleep in the 48 hours following intense eccentric work — find that DOMS becomes progressively shorter and less disruptive as both the physical adaptations of training and the habitual recovery practices combine to accelerate the resolution of each subsequent bout. This knowledge, consistently applied across the full arc of an athletic training life, compounds into the sustainable, enjoyable, high-performance fitness practice that is the real goal behind every individual workout, recovery protocol, and training decision.

Preventing DOMS and Training Smart: Protocols for Minimizing Soreness
Prevention is more effective than treatment for DOMS — the strategies that minimize initial DOMS severity reduce the recovery burden and training disruption that management requires. Prevention does not mean avoiding the training stimulus that causes DOMS, but structuring the training approach so that adaptation occurs progressively rather than requiring maximal initial soreness as the cost of beginning or changing a training program.
Progressive Volume Introduction: The Foundational Prevention Strategy
The most effective DOMS prevention is graduated progressive exposure — introducing novel exercises or significantly higher volumes in incremental steps that allow each exposure to build the repeated bout protection that reduces subsequent soreness before the next volume increase. The practical protocol for introducing a new exercise: week 1 — perform 2 sets at 60% of planned working weight; week 2 — 3 sets at 75%; week 3 — 3–4 sets at 90%; week 4 — full target volume at working weight. This 4-week ramp-up produces dramatically less cumulative DOMS than immediately performing full volume at full intensity, while producing equivalent adaptation outcomes because the graduated exposure is itself a sufficient progressive overload stimulus. For athletes returning from a training break — 2 weeks or longer — reducing initial training volume to 50–60% of pre-break levels regardless of subjective readiness prevents the severe DOMS that full-volume resumption produces in detrained muscles that have lost their repeated bout protection.
Warm-Up Optimization for DOMS Prevention
A thorough, progressive warm-up before high-DOMS-risk training sessions reduces the severity of subsequent soreness by preparing the muscles for the eccentric loading they will encounter. The warm-up mechanism: progressive loading during warm-up activates protective neural and mechanical responses in the muscle before the working sets begin — the gradual introduction of eccentric stress during warm-up sets initiates a mild repeated bout effect that reduces vulnerability to the working set loads. Evidence-based warm-up protocol for DOMS prevention: begin with 5 minutes of general cardiovascular activity (reduces muscle temperature sensitivity and improves tissue extensibility), followed by 3–4 progressive warm-up sets of the target exercise at 40%, 60%, 75%, and 85% of working weight — each set preparing the muscle for the next level of loading. This progressive loading warm-up takes 10–15 minutes but meaningfully reduces DOMS from the subsequent working sets compared to inadequate or absent warm-up.
Eccentric Training Protocols: Building Eccentric Resilience
One of the most effective long-term DOMS prevention strategies is deliberately developing eccentric strength and resilience through targeted eccentric training — exercises and training techniques that specifically challenge the eccentric phase to build the structural adaptations that reduce eccentric vulnerability. Slow-tempo training (4–6 second eccentric phases on standard exercises) progressively develops eccentric resilience in familiar exercises while maintaining the movement patterns that transfer to sport performance. Nordic hamstring curls — the highest eccentric hamstring loading exercise — are consistently used in injury prevention protocols (the Oslo Sports Trauma Research Center’s FIFA 11+ program) because their eccentric-focused stimulus develops the hamstring structural resilience that reduces both DOMS and hamstring strain injury risk. Accentuated eccentric training (using heavier loads for the eccentric phase than the concentric — requiring assistance on the concentric return) provides the highest eccentric loading stimulus but requires spotters or specialized equipment. The consistent principle: deliberate eccentric training progressively reduces both DOMS and injury risk from eccentric loading by building the structural adaptations that protect muscle from eccentric-induced damage.
Nutrition Timing for DOMS Prevention
Pre-exercise nutrition choices influence DOMS severity through their effects on the muscle’s metabolic state and inflammatory response capacity entering the training session. Pre-workout protein: consuming 20–30g of protein 1–2 hours before high-eccentric training provides the amino acid availability that supports rapid initiation of muscle protein synthesis immediately following the session — reducing the window of net protein breakdown that follows eccentric damage. Pre-workout antioxidants: there is theoretical concern (supported by some research) that high-dose antioxidant supplementation before training may blunt adaptation signals from exercise-induced reactive oxygen species — suggesting that routine high-dose vitamin C and E supplementation before training is counterproductive for long-term adaptation even if it reduces acute DOMS. Tart cherry juice consumed pre-exercise (4–5 days before a planned high-DOMS event, as in the protocol from section 3) reduces DOMS more effectively than post-exercise administration alone — confirming that pre-event nutritional preparation is part of the prevention toolkit, not just the recovery toolkit. Adequate glycogen stores: performing high-volume eccentric training in a glycogen-depleted state (from aggressive carbohydrate restriction or training fasted when depleted) may increase DOMS severity by limiting the energy availability for the repair processes that immediately follow the training session — adequate carbohydrate intake before planned high-DOMS-risk sessions is a practical prevention measure.
Programming Design to Minimize DOMS Disruption
Strategic training program design minimizes DOMS’s impact on overall training quality without reducing training stimulus. The key programming principles: sequence training sessions so that high-DOMS-risk exercises (new movements, high eccentric volume) are performed early in the training week, allowing the 3–5 day recovery window before the next high-demand session. Separate upper and lower body training so that DOMS in one region does not impair training quality in the other — leg DOMS does not prevent productive upper body training and vice versa. Reserve maximum-intensity, technique-demanding exercises for the first 1–2 sessions per week when DOMS from previous sessions is minimal — the sessions where full neuromuscular function is available for the highest-quality training stimulus. The weekly training template that minimizes DOMS disruption: Monday (high DOMS-risk lower body), Tuesday (upper body, lower body light active recovery), Wednesday (upper body high volume), Thursday (lower body, now reduced DOMS from Monday), Friday (full-body or weak-point focus). This structure allows each muscle group to recover sufficiently between high-DOMS-risk sessions while maintaining the training frequency that produces optimal adaptation.
When to Train Through DOMS vs. When to Rest
The training decision during active DOMS — whether to train the affected muscle group or rest it — is one of the most common practical questions athletes face, and the answer depends on DOMS severity and the type of training planned. Moderate DOMS (soreness noticeable but not limiting normal movement): training is appropriate and beneficial — the active recovery effect of light-to-moderate training on DOMS-affected muscles accelerates recovery while maintaining training consistency. The training adjustment: reduce load by 20–30%, avoid maximum effort sets, and prioritize range of motion and movement quality over maximal output. Severe DOMS (soreness that noticeably limits range of motion, causes compensatory movement patterns, or produces pain during non-maximal efforts): rest or active recovery only is appropriate for the affected muscle group — training severely DOMS-affected muscles at meaningful intensity increases injury risk from altered neuromuscular control without providing sufficient quality training stimulus to justify the additional damage. The decision heuristic: if you cannot move through the full range of motion of the target exercise without significant pain modification, the session is better used for active recovery, unaffected muscle group training, or mobility work — returning to full training for the affected group when soreness allows unimpaired movement quality.
Periodization and DOMS: Planning Soreness Into the Training Cycle
Advanced training periodization acknowledges DOMS as a predictable consequence of volume and intensity waves and plans training cycles accordingly — building high-volume, high-DOMS phases (accumulation blocks) followed by reduced-volume phases (intensification and deload blocks) that allow the cumulative DOMS debt from high-volume training to resolve before peak performance is required. The accumulation phase (weeks 1–4 of a training block): higher volume, more exercise variation, and deliberately higher DOMS exposure as the training load builds adaptation stimulus — this is the phase where introducing new exercises and volume increases is appropriate because the subsequent deload provides recovery. The intensification phase (weeks 5–8): volume reduces, intensity increases, exercise selection narrows to the highest-priority movements, and DOMS decreases as the training load becomes more specific and the volume per exercise reduces. The deload phase (week 9): volume drops to 40–60% of accumulation peak, allowing full resolution of any accumulated DOMS and fatigue before peaking or testing. This periodization approach front-loads the DOMS burden into the training phases where performance demands are lowest, and times the lowest DOMS and highest freshness for the phases where maximal performance is required. Athletes who understand periodization stop treating DOMS as an unwanted accident and start treating it as a planned training variable — strategically managed rather than reactively managed after the fact.
Sport-Specific DOMS Prevention: Application to Competitive Athletes
Competitive athletes require DOMS prevention strategies that maintain performance readiness at key competition periods while still allowing the high-volume training that builds fitness in preparation phases. The competition calendar governs training structure: high-DOMS-risk training (new exercises, volume peaks, high eccentric emphasis) is confined to the preparation phases that are temporally distant from key competitions, while the weeks immediately preceding competition use familiar exercises at lower volumes with minimal DOMS risk. The final 10–14 days before a major competition should produce minimal or zero DOMS — the taper phase of reduced volume at maintained or increased intensity specifically avoids the volume-induced DOMS that would impair peak performance. For team sport athletes who compete weekly, the training week structure must place high-DOMS-risk sessions 4–5 days from the next competition (typically immediately following the previous competition) to allow full resolution before the next performance requirement. This periodized, competition-calendar-aware approach to DOMS management is the standard in professional sport — the evidence-based application of the same principles available to recreational athletes who plan their training with awareness of their own performance calendar.
Mindset and DOMS: Reframing the Soreness Experience
The psychological relationship with DOMS — whether it is experienced as threatening evidence of damage or as reassuring evidence of productive training stimulus — meaningfully influences both the subjective severity of soreness and the behavioral response to it. Research on pain psychology consistently finds that catastrophizing interpretations of pain amplify subjective pain intensity through central sensitization mechanisms — athletes who interpret DOMS as “I damaged my muscles badly” experience greater functional impairment from equivalent soreness than athletes who understand DOMS as “my muscles are adapting to a new stimulus.” Reframing DOMS within an accurate physiological understanding — “this soreness is the inflammation phase of the adaptation process that will make my muscles stronger” — reduces catastrophizing and the anxiety-mediated central sensitization that amplifies DOMS beyond its underlying peripheral stimulus. This does not require ignoring severe soreness that might indicate injury, but it does mean developing the informed confidence to distinguish normal adaptive DOMS from pathological pain that warrants concern — and responding to the former with the appropriate management strategies rather than the anxious rest and avoidance that impairs both recovery and long-term training consistency.
The prevention strategies — progressive introduction, eccentric resilience development, warm-up optimization, nutritional preparation, and smart programming design — collectively reduce DOMS from an unavoidable training consequence into a manageable, strategically timed adaptive signal that occurs when planned and minimally disrupts performance when it matters most. Prevention strategies applied systematically across the training program — progressive introduction, eccentric resilience development, strategic programming design, and informed periodization — reduce DOMS from a chronic training disruption into a manageable, predictable component of the planned adaptation process. The athlete who understands DOMS at the mechanistic, strategic, and psychological level described in this article trains with the informed confidence that converts soreness from a barrier to consistent training into a familiar, manageable signal of productive adaptation — the mark of the evidence-informed, resilient athletic practice that produces long-term fitness results independent of the inevitable discomforts that progressive training always involves. The programming principles that minimize DOMS disruption — sequencing high-risk sessions early in the training week, separating upper and lower body training, reserving maximum-intensity efforts for the sessions with lowest preceding soreness — are equally valuable for performance optimization and for long-term training enjoyment, since consistently training with full neuromuscular function is both more productive and more satisfying than grinding through sessions compromised by residual soreness from poorly timed previous training. Train smart, recover well, and build the athletic resilience that makes DOMS a manageable stepping stone rather than a recurring obstacle.

DOMS Myths Debunked, When to See a Doctor, and Frequently Asked Questions
DOMS is surrounded by more persistent myths than almost any other fitness topic — misinformation that ranges from the long-debunked lactic acid theory to modern myths about foam rolling “flushing out” toxins. Clearing these myths matters because athletes who act on incorrect DOMS information make training decisions — resting when they should move, avoiding effective recovery strategies, using ineffective ones — that impair both their recovery and their long-term training progress.
DOMS Myths Debunked
Myth 1: DOMS is caused by lactic acid buildup. This is perhaps the most persistent fitness myth in existence — lactic acid (more accurately, lactate and hydrogen ions) is a byproduct of intense anaerobic exercise that clears from muscle tissue within 1–2 hours of exercise completion. DOMS peaks at 24–72 hours — long after lactate has completely cleared. The actual mechanism, as detailed in section 2, is eccentric-induced microstructural muscle damage followed by an inflammatory cascade. Myth 2: More DOMS means a better workout. DOMS indicates exercise novelty and eccentric loading stress — not workout quality, training effectiveness, or hypertrophy stimulus. Well-trained athletes performing highly effective workouts experience minimal DOMS because their muscles are adapted to the training stimulus. Chasing soreness as a proxy for effective training optimizes for the wrong variable. Myth 3: Stretching prevents or cures DOMS. Multiple systematic reviews on static stretching and DOMS find no meaningful effect of pre- or post-exercise stretching on DOMS severity or duration. Stretching has legitimate benefits for flexibility and range of motion, but DOMS prevention is not among them. Myth 4: Foam rolling flushes toxins from muscles. The mechanism of foam rolling’s DOMS benefit is increased local circulation and neurological pain modulation — not “toxin flushing,” which is not a physiologically coherent concept. Waste products of metabolism are removed by the venous and lymphatic systems, not by manual tissue pressure. Myth 5: You should always train through DOMS. Active recovery and light training on DOMS-affected muscles is evidence-supported and beneficial. Training at full intensity through severe DOMS that limits range of motion and produces compensatory movement patterns increases injury risk without meaningful training benefit. The appropriate response to DOMS is load-adjusted training, not either complete avoidance or willpower-based full-intensity training through functional impairment.
Ineffective DOMS “Remedies” to Skip
Several commonly recommended DOMS interventions lack meaningful research support. Static stretching: as noted above, consistently fails to reduce DOMS in research — stretch for flexibility, not for soreness. Alcohol: despite anecdotal claims, alcohol impairs muscle protein synthesis and the hormonal environment of recovery, making post-training alcohol consumption counterproductive for recovery regardless of any subjective pain-numbing benefit. Epsom salt baths: the theoretical mechanism (magnesium absorption through the skin reducing muscle soreness) is not supported by research on skin magnesium uptake — the warm bath itself (via mild heat and relaxation) may provide minor benefit, but magnesium absorption is not the mechanism. Compression-first cold therapy protocols without the recovery movement: ice application directly to DOMS-affected muscles without the circulation-supporting active recovery component reduces pain briefly but does not accelerate the underlying recovery process without the complementary blood flow increase that active recovery provides. These ineffective interventions are not harmful (most are neutral at worst) but represent opportunity costs — time and money spent on ineffective approaches that could be invested in the evidence-supported strategies that produce genuine benefit.
When to See a Doctor About DOMS
The vast majority of DOMS is self-limiting and requires no medical evaluation. Seek medical attention promptly if any of the following are present: dark or cola-colored urine following intense exercise (possible rhabdomyolysis requiring immediate evaluation), DOMS that worsens rather than progressively improves over 5–7 days, severe swelling with warmth and redness suggesting infectious process or significant hematoma, acute sharp pain during or immediately after exercise that precedes the soreness (possible acute muscle tear rather than typical DOMS), neurological symptoms (numbness, tingling, weakness) accompanying the soreness, or systemic symptoms (fever, chills, unusual fatigue) that suggest immune involvement beyond normal inflammatory response. Athletes with cardiovascular conditions should consult their physician before beginning high-intensity exercise programs that carry rhabdomyolysis risk, as impaired kidney function from pre-existing conditions increases susceptibility to exercise-induced acute kidney injury. The general principle: DOMS is bilateral, follows a predictable timeline (peaks at 48 hours, resolves by day 5–7), and is proportionate to the exercise performed — any presentation that deviates significantly from this pattern warrants professional evaluation to rule out pathology.
DOMS and the Long-Term Athletic Development Perspective
Across years of consistent training, the relationship with DOMS changes in ways that reflect genuine athletic development. The beginner who experiences dramatic DOMS from every new workout progressively develops the eccentric resilience and repeated bout protection that makes training increasingly comfortable — not because training becomes less effective, but because the musculoskeletal system adapts to handle the mechanical demands of regular training without requiring the same magnitude of inflammatory response. The experienced athlete who rarely experiences significant DOMS is not evidence of insufficient training stimulus — it is evidence of a well-conditioned musculoskeletal system that has developed the structural resilience to absorb training stress without the dramatic acute damage response of the unconditioned state. This progression — from frequent significant DOMS to rare, mild soreness from genuinely novel stimuli — is one of the most practically meaningful markers of athletic development, representing the accumulated structural adaptation of years of consistent progressive training.
Frequently Asked Questions About DOMS
How long does DOMS last? Typical DOMS from moderate eccentric exercise lasts 3–5 days, peaking at 24–72 hours and progressively resolving. Severe DOMS from extreme eccentric exercise (first marathon, very high-volume squat session for a beginner) may persist for 7–10 days. DOMS lasting beyond 7–10 days without progressive improvement warrants medical evaluation.
Is it safe to exercise with DOMS? Yes — with appropriate load adjustments. Light-to-moderate exercise on DOMS-affected muscles accelerates recovery through the active recovery mechanism. Reduce load by 20–30% and avoid maximum effort sets. Avoid training severely DOMS-affected muscles at full intensity when range of motion is limited.
Does DOMS get worse as you age? Evidence suggests older adults may experience similar peak soreness but slower resolution — the recovery timeline may extend from 3–5 days to 4–7 days in adults over 50. More conservative progressive volume increases and longer rest between high-DOMS-risk sessions appropriately account for this age-related recovery difference.
Why do my legs hurt more than my upper body after DOMS? Lower body exercises (squats, deadlifts, lunges) involve larger muscle masses under greater absolute loads and more pronounced eccentric loading than most upper body exercises — producing greater total muscle damage and typically more severe DOMS. The quadriceps and hamstrings are among the most DOMS-susceptible muscles in the body given their eccentric loading profile in most lower body training.
Can DOMS become permanent? No — DOMS is a transient inflammatory response that resolves completely. Chronic muscle soreness that does not follow the DOMS timeline (appearing 24–48 hours after specific exercise and resolving within 7 days) and does not correlate with training sessions is not DOMS and should be evaluated by a physician or physical therapist to identify the actual cause.
DOMS and Mental Toughness: Building Psychological Resilience Through Soreness
The experience of managing significant DOMS — continuing to train appropriately despite discomfort, maintaining perspective on the soreness as adaptive rather than threatening, and following through on the recovery protocols that accelerate resolution — develops a specific form of athletic psychological resilience that transfers to performance under pressure. Athletes who have navigated multiple significant DOMS periods develop the confident knowledge that soreness is finite, manageable, and followed by genuine strength improvements — converting what initially felt overwhelming into a familiar, navigable discomfort that no longer carries psychological threat. This accumulated experience of “I have been this sore before and recovered fully” is one of the most practically useful components of long-term athletic development — the embodied confidence in the body’s recovery capacity that allows athletes to push genuinely hard in training without the fear of the consequences that limits the training intensity of those who have not yet accumulated this experience. Treating DOMS management as a skills practice — learning the specific recovery interventions that work for your individual physiology, developing the training intuition to know when to reduce load and when to push through — builds the athletic self-knowledge that is one of the most valuable outcomes of years of consistent training, alongside the fitness adaptations that training directly produces.
DOMS in the Context of Overall Recovery Management
DOMS does not exist in isolation — it is one component of the broader recovery challenge that includes cumulative fatigue, sleep debt, nutritional deficits, and psychological stress that collectively determine an athlete’s recovery state and training readiness. Managing DOMS effectively requires the same integrated approach as managing overall recovery: adequate sleep (the single highest-impact recovery intervention for all dimensions of athletic recovery), appropriate nutrition (protein for muscle repair, carbohydrates for glycogen restoration, micronutrients for immune and enzymatic function), stress management (psychological stress impairs immune function and hormonal recovery environment), and strategic training structure (periodized volume that prevents excessive accumulated fatigue from overwhelming the body’s recovery capacity). The athlete who optimizes all dimensions of the recovery environment simultaneously — rather than focusing exclusively on DOMS-specific interventions while neglecting sleep, nutrition, or stress management — resolves DOMS faster and maintains higher training quality across the full training cycle than one who addresses DOMS in isolation. The comprehensive recovery approach that supports DOMS resolution is identical to the comprehensive recovery approach that supports optimal athletic performance — making DOMS management not a separate concern but an integrated component of the evidence-based training and recovery practice that all serious athletes should cultivate.
Building Your Personal DOMS Management Protocol
Every athlete’s DOMS experience is individual — different exercise types produce more severe soreness, different recovery interventions work more effectively, and different training histories create different vulnerability patterns. Building a personalized DOMS management protocol requires the deliberate self-experimentation and record-keeping that identifies which specific combination of prevention and recovery strategies works best for your individual physiology and training context. Track in your training journal: which exercises reliably produce significant DOMS, how many days until the soreness resolves, which recovery interventions produced the most noticeable relief, and how DOMS from the previous session affected training quality in the subsequent session. After 3–4 months of tracking, patterns emerge that guide personalized management — the athlete who discovers that tart cherry juice consistently reduces their DOMS duration by a day has genuinely useful individual evidence; the one who finds that ice baths make minimal difference but active recovery cycling provides substantial relief has equally valid personal data. This individualized evidence base, built from systematic observation of your own recovery responses, is ultimately more relevant than any general recommendation — because no general recommendation was developed specifically for your physiology, training history, and lifestyle context.
DOMS is not the enemy of athletic progress — it is the temporary price of the adaptation that makes athletes stronger, more resilient, and more capable over time. Managing it intelligently, rather than fearing it or ignoring it, is the mark of the experienced, evidence-informed athlete. The athlete who understands DOMS at the mechanistic, strategic, and psychological level described in this article trains with the informed confidence that converts soreness from a barrier to consistent training into a familiar, manageable signal of productive adaptation — the mark of the evidence-informed, resilient athletic practice that produces long-term fitness results independent of the inevitable discomforts that progressive training always involves. The comprehensive DOMS guide in this article — from the physiological mechanisms through the evidence-based recovery strategies, prevention protocols, myth debunking, and personalized management framework — provides every tool an athlete needs to transform their relationship with soreness from anxious avoidance or uninformed endurance into the intelligent, evidence-based management practice that makes DOMS a temporary, manageable component of productive athletic training rather than a recurring barrier to training consistency and performance. Every athlete who commits to understanding and managing DOMS as described in this article will train more consistently, recover more effectively, and build more durable athletic capacity than one who treats soreness as an obstacle to endure rather than a signal to interpret and manage.





