
What to Do If You Feel a Sharp Pain During Exercise
⚠️ Disclaimer: The information in this article is for general educational purposes only and does not constitute medical, nutritional, or professional fitness advice. Individual results may vary. Always consult a qualified healthcare professional or certified fitness trainer before starting any new exercise program, changing your diet, or making decisions about injury treatment or recovery. If you experience pain, discomfort, or any unusual symptoms during exercise, stop immediately and seek professional guidance.

Understanding Sharp Exercise Pain: What Your Body Is Telling You
Sharp pain during exercise is one of the clearest signals the body produces — and one of the most frequently misinterpreted. The fitness culture’s “no pain, no gain” narrative has created a generation of athletes who push through pain signals that their nervous system is generating for critical protective reasons, resulting in the acute injuries, stress fractures, tendon ruptures, and joint damage that training through pain produces. Conversely, pain anxiety causes many athletes to stop beneficial training at the first sensation of discomfort — confusing the beneficial metabolic stress of hard training with the warning signal of genuine tissue damage. The ability to distinguish between these two categories of pain signal — the discomfort of productive training stress versus the warning of genuine tissue threat — is one of the most valuable practical skills an athlete can develop, and this article provides the complete framework for making that distinction accurately and responding appropriately to each type of signal.
The Pain Classification System Every Athlete Needs
Sports medicine clinicians use a refined pain classification framework that distinguishes between types of pain by their quality, location, onset pattern, and associated symptoms — providing the clinical basis for the immediate response decisions that the type of pain signal demands. Type 1: Muscle burn (metabolic discomfort). The deep, diffuse burning sensation in working muscles during high-intensity effort — the lactic acid accumulation and hydrogen ion production that intense exercise generates. This is the productive discomfort of effective training: it is bilateral when both limbs are working equally, proportional to exercise intensity, located diffusely within the working muscle belly rather than at a specific point, and resolves within seconds to minutes of effort reduction. This pain type is not only safe to train through — it is the signal that the training stimulus is sufficient to drive adaptation. Type 2: DOMS (delayed onset muscle soreness). The diffuse, tender muscle soreness appearing 12–48 hours after eccentric-dominant or novel exercise — the inflammatory response to the microtrauma that produces muscle adaptation. DOMS is appropriate for training through with reduced intensity and is not associated with injury risk. Type 3: Joint discomfort (acceptable). The mild achiness that some athletes experience in chronically used joints during warm-up, typically resolving within 10–15 minutes of movement. Generally safe to continue training once the discomfort resolves during warm-up — but should be monitored and investigated if persistent. Type 4: Sharp, localized pain (warning signal). The sudden, specific, often shocking pain that demands immediate attention — the signal that acute tissue loading has exceeded the structural tolerance of a specific tissue at a specific location. This is the pain type this article addresses. Sharp pain is characterized by: sudden onset (often during a specific movement or at a specific point in a movement); precise location (the athlete can point to the exact spot with one finger); high intensity (often 6–10 on a pain scale, difficult to ignore); and often associated with immediate functional loss (the limb or region cannot perform the movement that preceded the pain without significant pain reproduction). Type 5: Referred pain (potential serious pathology). Pain in a location distant from the apparent source — chest pain radiating to the left arm and jaw during exertion, shoulder pain that is actually cardiac in origin, or leg pain arising from lumbar nerve compression. Referred pain patterns should always be investigated medically, as they indicate pathology at a site distant from where the pain is felt.
The Neuroscience of Pain: Why Your Brain Creates Pain Signals
Pain is not a direct measure of tissue damage — it is a protective response generated by the brain based on threat assessment of information from peripheral nociceptors (danger detectors in tissues), prior pain experiences, current emotional and psychological state, contextual factors, and the brain’s assessment of the biological danger that the current situation represents. This neuroscience understanding has practical athletic implications: the same level of tissue stress can produce dramatically different pain experiences depending on context — a paper cut in everyday life produces significant pain; the same wound received in an intense athletic competition may not be noticed until afterward because the brain’s threat assessment is suppressed by the competitive context and adrenaline. Sharp pain during exercise, despite its psychological complexity, reliably indicates one of two scenarios: genuine acute tissue overload (a muscle, tendon, ligament, or joint structure has been stressed beyond its current structural capacity — a genuine injury signal that demands immediate response); or neural sensitization (a previously injured or chronically stressed tissue has lowered the threshold for pain signal generation, producing sharp pain at loading levels that would not produce pain in non-sensitized tissue — a genuine signal that requires load modification and professional assessment, even though the pain level exceeds the actual tissue damage). From the British Journal of Sports Medicine on pain assessment guidelines, the appropriate initial response to sharp exercise pain is the same regardless of the suspected underlying mechanism: stop the provocative activity, assess the pain characteristics, and make the continue/stop decision based on the specific pain type and associated findings described in this article.
Sharp Pain vs. Productive Discomfort: The Decision Framework
The practical decision framework for distinguishing sharp pain from productive discomfort uses five assessment criteria that can be applied in real time during a training session: Location specificity (can you point to the exact spot with one finger? — sharp pain is localized; productive discomfort is diffuse); Onset pattern (did the pain arrive suddenly during a specific movement? — sharp pain has sudden onset; productive discomfort builds gradually with effort); Pain quality (is the sensation sharp, stabbing, or electric? — sharp pain has these qualities; productive discomfort is burning, aching, or heavy); Functional impact (does the pain prevent normal movement of the affected body part? — sharp pain often produces immediate functional limitation; productive discomfort does not); and Associated symptoms (does the pain come with swelling, joint instability, numbness, or unusual sounds? — these are red flags for genuine tissue damage that productive discomfort never produces). Score: if three or more of these five criteria indicate sharp pain, stop the training activity immediately and proceed to the acute response protocol in Section 3. If two or fewer criteria indicate sharp pain, reduce intensity, monitor for one set, and reassess. This framework is not infallible — when in doubt, always err on the side of stopping. The training session lost to caution is recovered in days; the injury that results from training through genuine sharp pain may require weeks to months of recovery.
The Psychological Dimension: Fear of Pain and Training Avoidance
The psychological response to sharp exercise pain — particularly in athletes who have experienced previous significant injuries — can produce pain catastrophizing and kinesiophobia (fear of movement) that impair athletic function far beyond the actual tissue damage the injury caused. Pain catastrophizing: the tendency to magnify the threat of pain, ruminate on pain, and feel helpless in the face of pain — producing training avoidance that prevents the progressive reloading that tissue healing requires and perpetuates the deconditioning that makes re-injury more likely. Kinesiophobia after acute sharp pain injury: the fear that movement will cause re-injury reduces training participation, alters movement patterns (compensatory movement that overloads healthy tissue to protect the injured site), and produces the disuse atrophy that extends the rehabilitation timeline beyond what the original injury required. The evidence-based psychological approach to sharp pain recovery: early graded re-exposure to the provocative movements (within pain-free ranges, progressively loaded) prevents the kinesiophobia that complete avoidance produces; pain education (understanding that pain is a protective signal rather than an accurate measure of tissue damage) reduces catastrophizing; and setting specific, progressive return-to-training milestones provides the goal framework that replaces vague fear of re-injury with concrete, achievable steps toward full recovery. Athletes who understand the neuroscience of pain — that sharp pain is a threat signal generated by the brain, not a direct readout of tissue destruction — are better equipped to engage in the graded progressive rehabilitation that full recovery requires without being derailed by the normal pain fluctuations that tissue healing produces.
Sharp exercise pain is the body’s urgent signal — the athlete who responds to it with knowledge and protocol, rather than bravado or panic, protects both the training session and the long-term athletic career that intelligent pain management sustains. The tools in this article provide exactly that knowledge. Apply them consistently, share them with training partners who need them, and build the pain-intelligent training culture that competitive and recreational athletes at every level benefit from. Your long-term athletic development depends on it — and the sharp pain episode that prompted reading this article may prove to be the most valuable training lesson you ever receive. Every sharp pain episode, managed correctly, makes the athlete stronger, wiser, and more resilient than before. That is the ultimate lesson of pain in athletic training.
The Most Common Causes of Sharp Pain During Exercise
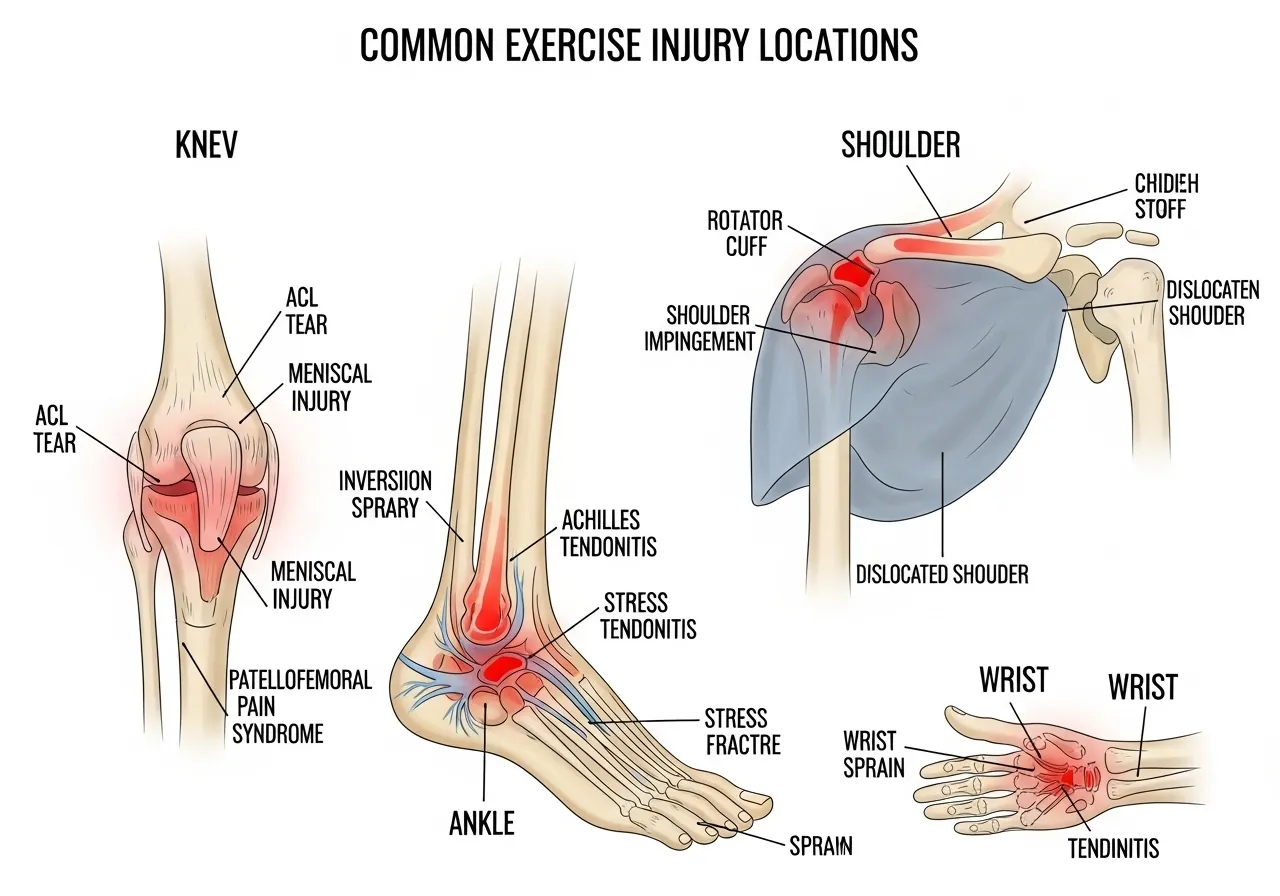
Sharp exercise pain arises from a limited number of anatomical sources — each with characteristic presentation patterns that allow preliminary identification during the workout and guide the appropriate response and subsequent management. This section covers the eight most common causes of acute sharp exercise pain, with the distinguishing features that help athletes recognize which structure is likely involved.
Muscle Strains: The Most Common Acute Sharp Pain Source
Muscle strains — tears of muscle fibers ranging from microscopic (Grade 1) to complete muscle belly rupture (Grade 3) — are the most common cause of sudden sharp pain during exercise, particularly during high-velocity movements, maximal effort contractions, or rapid direction changes. The characteristic presentation: sudden sharp pain in the muscle belly during a specific movement (most commonly sprinting for hamstring strains, throwing for rotator cuff strains, or heavy lifting for quadricep or pectoral strains); immediate functional limitation (difficulty contracting the muscle against resistance); local tenderness on palpation; and progressive swelling and bruising over 24–48 hours for Grade 2–3 strains. The most commonly strained muscles in athletes: hamstrings (typically at the proximal musculotendinous junction — the sharp pain at the back of the thigh during sprinting or kicking); quadriceps (particularly the rectus femoris in kicking sports); gastrocnemius (the “tennis leg” — sharp calf pain during push-off, more common in masters athletes); and pectoral muscles (during bench press or throwing, producing sharp anterior chest pain). Grade 1 strains (microscopic tearing — mild pain, minimal functional loss, return to training in 3–7 days with appropriate management) are the most common and least serious; Grade 3 strains (complete rupture — severe pain, significant functional loss, palpable defect in the muscle, requiring surgical assessment) are fortunately rare in recreational athletes.
Ligament Sprains and Joint Injuries
Ligament sprains — tears of the connective tissue that stabilizes joints — produce sharp joint pain, often accompanied by the “pop” or “crack” that audible ligament failure produces. The knee ligaments (anterior cruciate ligament — ACL, medial collateral ligament — MCL) and ankle ligaments (anterior talofibular — ATFL, calcaneofibular — CFL) are the most commonly sprained in recreational athletes. ACL injury presentation: sudden sharp knee pain, often accompanied by a felt or heard “pop,” immediate significant swelling (hemarthrosis — bleeding into the joint), and profound knee instability (the knee “giving way”). The mechanism: non-contact deceleration, cutting, or landing movements that place the knee in valgus with internal tibial rotation — the loading pattern that exceeds ACL tensile strength. ACL injury requires immediate medical evaluation, imaging, and orthopedic consultation — the sharp knee pain from a suspected ACL mechanism should prompt exercise cessation and emergency medical assessment, not a “wait and see” approach. Ankle sprain presentation: sharp lateral ankle pain from an inversion (rolling outward) mechanism, rapidly developing swelling over the outer ankle, and pain on weight bearing. Grade 1–2 ankle sprains (the majority of ankle sprains) respond well to the PEACE and LOVE protocol (described in Section 5) without requiring imaging in most cases. The Ottawa Ankle Rules — validated clinical guidelines for determining when ankle X-ray is required — should be applied when ankle sprain severity is uncertain.
Tendon Issues, Nerve Pain, and Bone Stress
Tendinopathy (chronic tendon degeneration) and acute tendon tears produce a characteristic sharp pain at the tendon insertion or midsubstance — most commonly at the Achilles tendon, patellar tendon, rotator cuff tendons, and common extensor origin at the elbow (lateral epicondyle). The Achilles tendon tear presentation: sudden sharp pain at the back of the ankle during explosive push-off (described as feeling like being kicked from behind), immediate inability to plantar-flex against resistance, and a palpable gap in the tendon in complete ruptures — requiring immediate surgical consultation. Nerve impingement produces the sharp, electric, shooting pain that distinguishes it from musculoskeletal sources — the pain travels along the nerve distribution rather than remaining localized to one point. The common nerve impingement presentations during exercise: lumbar disc herniation with nerve root compression (sharp shooting pain from the low back into the leg, often with numbness or tingling in the dermatomal distribution); carpal tunnel syndrome (sharp wrist and hand pain during weight-bearing exercises); and piriformis syndrome (sharp buttock pain with sciatica-like radiation). Bone stress injuries — stress reactions and stress fractures from repetitive loading that exceeds the bone remodeling capacity — present as progressively worsening localized sharp bone pain that is worst with impact loading and improves with rest. The tibia, metatarsals, and navicular are the most common sites in runners. From Journal of Orthopaedic and Sports Physical Therapy pain guidelines, bone stress injuries require imaging confirmation (MRI is more sensitive than X-ray for early stress reactions) and load modification before medical clearance to resume impact training.
Cardiac and Visceral Sources: The Red Flag Pain Patterns
A small but critically important proportion of exercise-induced sharp pain originates from cardiac, pulmonary, or abdominal visceral sources rather than the musculoskeletal system — and these sources require immediate emergency medical response rather than the sports medicine management that musculoskeletal pain demands. The cardiac emergency presentation during exercise: sharp or crushing chest pain, pressure, or tightness (any quality of chest discomfort during exertion must be treated as a potential cardiac emergency until proven otherwise); pain radiating to the left arm, jaw, or back; associated symptoms of shortness of breath, sweating, nausea, or dizziness; and sudden unexpected extreme fatigue. This constellation of symptoms during exercise constitutes a medical emergency requiring immediate cessation of activity, calling emergency services, and remaining in a safe position until help arrives. Exercise-induced bronchospasm (exercise-induced asthma) produces sharp chest tightness and breathlessness during or after intense exercise — not typically the localized sharp pain of musculoskeletal origin, but distressing enough to be confused with cardiac or musculoskeletal sources. Side stitches (exercise-related transient abdominal pain — ETAP) produce sharp sub-diaphragmatic pain during running or aerobic exercise — benign and resolving quickly with pace reduction and breathing techniques, but occasionally confused with splenic or hepatic pain in athletes unfamiliar with this common phenomenon. Any exercise-associated sharp pain in the chest, upper left arm, jaw, or between the shoulder blades — particularly in athletes with cardiovascular risk factors (hypertension, diabetes, family history of cardiac disease) — requires emergency medical assessment before any return to exercise.
Recognizing the type of pain accurately is the most valuable exercise-related skill an athlete develops over time.

How to Respond When Sharp Pain Strikes Mid-Workout
The immediate response to sharp exercise pain — the decisions made in the seconds and minutes following the pain onset — significantly determines the severity of the injury that results, the recovery duration, and the probability of further tissue damage from continued loading. This section provides the stepwise acute response protocol that all athletes should know and execute automatically when sharp pain occurs.
The Immediate Stop-Assess-Decide Protocol
Step 1 — Stop immediately: at the onset of sharp, localized exercise pain, stop the provocative movement immediately. Do not complete the set, do not attempt one more rep to “see if it was a fluke.” The neural pain signal precedes tissue failure — the sharp pain is the warning that the tissue is at or near its structural limit, and continued loading after this signal risks converting a Grade 1 strain or a stress reaction into a Grade 2–3 tear or complete stress fracture. The athletic instinct to push through is the primary driver of acute injury severity escalation — overriding it with the immediate stop response is the single most impactful acute injury prevention behavior. Step 2 — Assess the pain characteristics using the framework from Section 1: localized or diffuse? Sharp or burning? Sudden onset or gradual? Functional limitation present? Associated symptoms (swelling, instability, numbness, audible sounds)? This rapid assessment takes 30–60 seconds and provides the information needed for the Step 3 decision. Step 3 — Decide: if the pain is sharp, localized, associated with functional limitation or significant severity (6+/10), or accompanied by red flag symptoms (cardiac presentation, audible pop with significant joint instability), stop training entirely and proceed to the appropriate response (ice, elevation, medical assessment as indicated). If the pain is mild, diffuse, and without functional limitation, reduce intensity and reassess after 5 minutes — if the pain is resolving, continue training at reduced intensity with careful monitoring; if unchanged or worsening, stop training.
PEACE and LOVE: The Modern Acute Injury Protocol
The PEACE and LOVE protocol — developed by sports medicine researchers as an update to the outdated RICE (rest, ice, compression, elevation) framework — provides evidence-based acute and subacute injury management guidance that optimizes tissue healing. PEACE (days 1–3, acute phase): Protection (avoid movements that cause pain, use assistive devices if weight-bearing is painful — but complete rest is rarely indicated for most soft tissue injuries); Elevation (elevate the injured limb above heart level to reduce the hydrostatic pressure that drives swelling formation — most effective in the first 24–48 hours); Avoid anti-inflammatory modalities (the inflammatory response is the first phase of tissue healing — NSAIDs and ice inhibit the inflammation that necessary for initiating the healing cascade; current evidence recommends avoiding both NSAIDs and ice for the first 72 hours of most soft tissue injuries, in contrast to the RICE protocol’s ice recommendation); Compression (elastic bandage compression reduces swelling volume and provides proprioceptive support that reduces reinjury risk during early return to movement — apply firmly but not so tightly as to restrict circulation); Education (understand that pain is a protective signal, that tissue healing follows a predictable timeline, and that graded progressive loading within pain tolerance is the evidence-based rehabilitation approach). LOVE (days 3–14, subacute phase): Load (early controlled loading within pain tolerance — the mechanical stimulus that promotes organized collagen synthesis and appropriate scar tissue formation, preventing the disorganized scar that complete rest produces); Optimism (positive expectations about recovery outcomes are associated with faster return to full activity — pain catastrophizing is associated with delayed recovery); Vascularization (aerobic exercise that does not provoke the injury — swimming for lower limb injuries, cycling for upper limb injuries — maintains cardiovascular fitness and promotes healing through increased blood flow); Exercise (progressive range of motion and strengthening exercises within pain tolerance — the rehabilitation that restores the strength and movement quality the injury has disrupted). From ACSM injury management guidelines, the PEACE and LOVE protocol represents the current best-practice standard for most soft tissue injuries encountered during exercise.
The Return-to-Training Decision: Criteria for Safe Exercise Resumption
Premature return to training after sharp exercise pain injury is the primary driver of re-injury, which consistently produces more severe tissue damage and longer recovery than the original injury. The evidence-based return-to-training criteria: full range of motion compared to the unaffected side (or pre-injury baseline for bilateral structures); pain-free performance of the activity that provoked the original injury at low to moderate intensity; strength at 90% or greater compared to the unaffected side (assessed through functional testing for limb injuries); and no swelling or warmth at the injury site after training. These criteria should be met in sequence across progressive intensity levels — pain-free at walking before running, pain-free at bodyweight before loaded exercise, pain-free at moderate loads before maximum effort. The graduated return-to-training timeline for common injuries: Grade 1 muscle strains 3–7 days with appropriate management; Grade 2 muscle strains 2–6 weeks; Grade 1–2 ankle sprains 3–21 days depending on severity; patellofemoral pain 2–6 weeks of load modification before progressive return; rotator cuff tendinopathy 6–12 weeks of progressive rehabilitation. These timelines assume appropriate management and active rehabilitation — passive rest without progressive loading consistently produces longer recovery times than the active rehabilitation approach.
Implement the protocols in this article and train with lasting confidence.

Injury Prevention: Stopping Sharp Pain Before It Starts
Sharp exercise pain is largely preventable — the majority of acute exercise injuries occur in contexts where identifiable risk factors were present and modifiable before the injury occurred. Systematic injury prevention addresses the structural weaknesses, movement pattern errors, training load errors, and warm-up deficiencies that create the conditions for acute tissue overload.
Training Load Management: The Primary Injury Prevention Tool
Sudden increases in training load — volume, intensity, or frequency changes that exceed the tissue’s adaptive capacity — are the primary driver of overuse injury and the most significant controllable risk factor for acute injury in athletes whose tissues are fatigued, underrecovered, or incompletely adapted to their current training demand. The acute-to-chronic workload ratio (ACWR): the ratio of the current week’s training load to the rolling 4-week average load provides a validated injury risk indicator. An ACWR above 1.5 (this week’s load is 50% higher than the recent average) is associated with significantly elevated injury risk in team sport athletes — the tissue is being loaded at a level it is not conditioned for, exceeding its structural tolerance. The practical application: limit week-to-week training load increases to 10% of the previous week’s load (the 10% rule, though research suggests the optimal threshold may be closer to 15% for well-conditioned athletes). Plan deload weeks (25–50% load reduction) every 4–6 weeks to allow the cumulative tissue fatigue from progressively increasing loads to resolve before the next loading block begins. Monitor subjective training readiness daily — consistently low readiness ratings (fatigue, poor sleep, low motivation) indicate accumulated fatigue that warrants load reduction before injury intervenes to impose it. From PubMed research on exercise injury prevention, training load management is consistently identified as the modifiable factor with the largest impact on injury incidence across all athletic populations.
Warm-Up, Mobility, and Movement Quality
The structured warm-up — progressively increasing tissue temperature and blood flow, activating the neuromuscular patterns that the training session requires, and identifying any pre-existing pain or movement restriction before full loading begins — is the accessible injury prevention practice that research consistently validates and athletic populations consistently under-utilize. The evidence-based warm-up structure: 5 minutes of light cardiovascular activity (elevating core temperature and increasing synovial fluid viscosity in joints); 5 minutes of dynamic mobility (leg swings, arm circles, hip circles, thoracic rotation — moving joints through their full range of motion with progressive speed and amplitude); 5 minutes of movement-specific activation (bodyweight versions of the training session’s primary movements, progressively approaching session intensity). The FIFA 11+ warm-up program — developed for football injury prevention but validated across multiple sports — reduces acute injury incidence by 30–50% in athletic populations that implement it consistently. Movement quality assessment during warm-up: if a movement feels “off,” restricted, or produces mild discomfort during the warm-up, investigate before loading it in the session. The athlete who notices limited hip flexion range during the warm-up squat and proceeds immediately to heavy barbell squats without addressing the restriction is creating the loading conditions for the sharp hip pain that the movement restriction will eventually produce under load. Identifying and addressing movement restrictions during the warm-up — even briefly, with a targeted stretch or mobility exercise — prevents the movement compensations under load that produce injury at vulnerable tissues.
Strength and Stability: The Structural Protection Approach
Tissue strength — both of the primary muscles and of the stabilizing muscles that protect joints from excessive force — is the structural protection against acute injury under maximal loading conditions. Strength imbalances between opposing muscle groups (quadricep-to-hamstring strength ratio below 0.6 in athletes predicts hamstring strain risk; hip abductor weakness predicts knee valgus and ACL injury risk in female athletes; rotator cuff weakness predicts shoulder impingement and labral injury in overhead athletes) create the neuromuscular vulnerabilities that maximal effort exposes. The injury prevention strength work that all athletes should include: hamstring curls and Romanian deadlifts for hamstring strain prevention; hip abduction and external rotation exercises (clamshells, lateral band walks, single-leg squats) for knee valgus and ACL injury prevention; rotator cuff external rotation and face pulls for shoulder injury prevention in pressing athletes; and single-leg balance and proprioception training for ankle sprain prevention. These exercises require 10–15 minutes added to 2–3 training sessions per week — an investment that research consistently identifies as producing significant injury risk reduction across all athletic populations. The Nordic hamstring curl — an eccentric hamstring exercise performed by kneeling and lowering the torso toward the floor under hamstring control — is the single exercise with the strongest evidence for hamstring strain prevention, reducing strain incidence by 50–70% in football and running athletes who perform it consistently.
Equipment, Surface, and Environmental Factors
The equipment and environment in which training occurs contribute to acute injury risk in ways that athletes frequently overlook. Footwear: training shoes that are appropriate for the training surface and movement pattern (cushioned running shoes for road running, stability shoes for athletes with overpronation, flat shoes for heavy strength training that requires ground contact stability) reduce the joint loading patterns that inappropriate footwear exacerbates. Shoes with excessive wear — visible compression of the midsole, worn-down outsoles, or breakdown of the heel counter — lose the support and shock absorption that injury prevention requires; replacing training footwear every 500–800km of running or when visible wear appears maintains the protective function that new footwear provides. Training surface: transitioning from soft training surfaces (grass, rubber track, treadmill) to hard surfaces (road, concrete) too rapidly is a common stress fracture and acute joint injury risk factor — the higher impact forces of hard surfaces require gradual adaptation over weeks rather than immediate full adoption. Equipment fit: resistance training equipment (barbells with worn knurling, cables with fraying, machines with incorrect seat height for the individual’s anthropometry) creates the movement compensations and unexpected load variations that acute injury occasions. Inspect training equipment regularly and report or address deficiencies before training on them. Temperature and humidity: cold environments reduce muscle flexibility and neural conduction speed, increasing acute muscle strain risk — the warm-up is more critical in cold environments and should be extended to ensure genuine core temperature elevation before full-intensity loading. Hot and humid environments increase the cardiovascular and thermoregulatory load of training, reducing the tissue tolerance for mechanical loading at equivalent subjective effort — reducing training intensity in extreme heat is injury prevention, not weakness.
Periodization and Recovery: Structuring Training to Prevent Overload
Periodization — the systematic variation of training load, intensity, and volume across planned time periods — is the most sophisticated and evidence-based approach to preventing the cumulative overload that produces both overuse injury and the conditions for acute sharp pain episodes. The athlete who trains at consistently high intensity without planned variation accumulates tissue fatigue faster than recovery can restore structural integrity — eventually reaching the point where a single training session that would be tolerable with fresh tissue produces acute failure in the fatigued state. Linear periodization (gradual progressive increase in load over a training block with periodic deload weeks) provides the structural variation that prevents cumulative overload: 3 weeks of progressive loading followed by 1 week of 50% volume reduction at maintained intensity allows tissue remodeling and structural repair that progressive loading without recovery cannot achieve. The block periodization approach (alternating between accumulation blocks emphasizing volume and intensification blocks emphasizing intensity, separated by realization or deload blocks) provides more sophisticated variation that advanced athletes use to both maximize performance development and minimize injury risk across longer training cycles of 12–24 weeks. The simple monitoring tool that operationalizes periodization for athletes without a coach: the daily readiness rating — rate overall readiness on a 1–10 scale each morning before training (considering sleep quality, muscle soreness, motivation, and general energy). Consistently low readiness ratings (below 5/10 for 3+ consecutive days) indicate accumulated fatigue that warrants a spontaneous deload — reducing planned training volume by 40–50% until readiness ratings recover to 7+/10. This responsive periodization approach uses subjective readiness as the primary load management signal rather than fixed periodization schedules that ignore the day-to-day variability of recovery quality that lifestyle factors (sleep, stress, nutrition, illness) produce.
Proprioception and Neuromuscular Control: The Hidden Injury Prevention Factor
Proprioception — the sensory system that informs the central nervous system of joint position, movement speed, and force production in real time — is the neuromuscular mechanism that prevents acute sharp pain injuries by automatically recruiting stabilizing muscles before a joint is loaded to the point of structural failure. Athletes with impaired proprioception — either from previous injury (proprioceptive deficits after ankle sprains are well documented and significantly predict sprain recurrence), insufficient balance training, or general athletic inexperience — lack the automatic neuromuscular protection that catches unexpected loading variations before they produce tissue damage. Proprioceptive training for injury prevention: single-leg balance exercises (progressing from flat stable surface to unstable surfaces such as balance discs or BOSU balls, adding upper limb challenges and perturbations to progress further) train the ankle and knee proprioceptive reflexes that prevent the loss of joint control that acute ligament sprains require; reactive agility drills (responding to random directional cues with cutting and direction change movements) train the neuromuscular response time that unexpected loading situations demand; and perturbation training (a training partner or therapist providing unexpected pushes or load changes during otherwise controlled exercises) trains the stabilizing muscle co-contraction patterns that prevent joint injury under sudden unexpected forces. Research on balance and proprioception training for injury prevention in team sport athletes consistently demonstrates 30–50% reduction in ankle sprain and knee injury incidence — benefits that require only 10–15 minutes of dedicated proprioception work added to 2–3 training sessions per week to achieve. This relatively small time investment produces injury prevention outcomes that dwarf the time cost when measured against the training time lost to the injuries it prevents.
Nutrition for Injury Prevention and Tissue Resilience
Nutritional status significantly influences tissue structural integrity and the tissue remodeling capacity that training adaptation requires — athletes with suboptimal nutrition for their training demands are at higher acute and overuse injury risk than equivalently trained athletes with nutritional support adequate for their training load. The key nutritional factors for injury prevention: protein (1.6–2.2g per kg of body weight provides the amino acids that muscle, tendon, and ligament remodeling requires — protein deficiency impairs collagen synthesis that tendon and ligament adaptation depends on); collagen precursors (10–15g of hydrolyzed collagen or gelatin consumed 30–60 minutes before training, with 200mg of vitamin C, provides the amino acids — particularly glycine, proline, and hydroxyproline — that stimulate collagen synthesis in tendons and ligaments during the post-exercise period when collagen synthesis is most elevated); vitamin D (deficiency impairs muscle function and bone mineral density, increasing acute muscle injury and stress fracture risk — athletes training in low-sunlight environments should monitor vitamin D status and supplement as needed); calcium (essential for bone structural integrity — athletes in caloric deficit or with restricted dairy intake may have insufficient calcium for the bone remodeling that training demands); and omega-3 fatty acids (EPA and DHA from fish oil at 2–3g per day reduce the chronic low-grade inflammation that tendinopathy development is associated with, and may reduce the cumulative inflammatory burden that repeated training produces). The nutrition for injury prevention is largely aligned with the general sports nutrition recommendations for performance and recovery — ensuring adequate total caloric intake is the most critical factor, as energy availability restriction impairs all tissue remodeling processes simultaneously and is the single most potent nutrition-related injury risk factor in athletic populations.
Train smart, recover fully, and stay injury-free for life.

Treatment and Recovery: What to Do After a Sharp Pain Episode
The 72 hours following a sharp exercise pain episode determine the trajectory of recovery — optimal management during this window reduces swelling, prevents secondary tissue damage, initiates the healing cascade, and sets up the progressive rehabilitation that restores full function. This section provides the complete evidence-based management protocol from immediate post-injury through return to full training.
Acute Phase Management (Hours 1–72)
Immediately following sharp exercise pain that results in exercise cessation: protect the injured area from further loading (use crutches if weight-bearing on an injured lower limb is painful; avoid overhead activities for shoulder injuries; support the wrist with a brace or wrap for wrist injuries); elevate the injured limb above heart level to reduce swelling; apply compression with an elastic bandage to limit swelling volume; and reassess pain and function over the first 24 hours to determine whether medical assessment is required. The ice controversy: the traditional RICE protocol’s ice recommendation has been challenged by current research — while ice reduces pain effectively (through nerve conduction slowing), it also inhibits the inflammatory response that initiates tissue healing. Current sports medicine guidance recommends ice for pain management if needed (not exceeding 15–20 minutes per application, not applied directly to skin) while acknowledging that it may slightly extend healing time. Athletes who prioritize pain management over fastest healing (competitive athletes who need to function during the injury) may choose ice for its analgesia; athletes who prioritize fastest healing (recreational athletes without competitive obligations) may prefer to avoid ice during the first 72 hours. NSAIDs (ibuprofen, naproxen): similarly, while effective for pain and swelling management, NSAIDs inhibit prostaglandin-mediated inflammation that is necessary for tendon and muscle healing — current guidance recommends avoiding NSAIDs during the first 72 hours of soft tissue injury if possible, using them sparingly thereafter for pain management rather than as a routine treatment. Paracetamol (acetaminophen) provides pain management without the anti-inflammatory effects that interfere with healing — it is the preferred analgesic during the acute healing phase for athletes who require pharmacological pain management.
Subacute Rehabilitation Phase (Days 3–21)
The subacute phase — from day 3 through approximately 3 weeks post-injury for most soft tissue injuries — is the critical rehabilitation window where early controlled loading promotes optimal tissue healing and prevents the disuse atrophy that complete rest produces. The progressive loading principle: begin movement within pain-free range on day 3, progressively increasing the range and then the resistance as pain tolerance allows, with the pain during exercise not exceeding 3–4/10 and resolving within 24 hours of each session (indicating that the loading is within the tissue’s healing tolerance). The progressive loading protocol for a hamstring strain example: day 3–5, gentle range of motion exercises (knee flexion and extension through comfortable range while supine); day 5–7, walking without limp as pain allows; day 7–10, slow jogging on flat surface if pain-free at walking; day 10–14, progressive running speed and straight-line acceleration; day 14–21, direction change and sport-specific movements at increasing intensity. This timeline is for Grade 1 strains — Grade 2 strains require doubling these timescales, and Grade 3 injuries require surgical consultation before rehabilitation planning. Manual therapy (sports massage, joint mobilization) provided by a qualified physiotherapist during the subacute phase reduces scar tissue adhesion formation, improves tissue extensibility, and accelerates the return of normal range of motion — professional physiotherapy assessment is strongly recommended for any acute sharp pain injury that does not show clear improvement within 5–7 days of self-management.
Chronic Phase: Returning to Full Training and Preventing Recurrence
The return to full training following acute sharp exercise pain injury is the phase where recurrence risk is highest — the partially healed tissue has not yet regained the full strength and neuromuscular coordination of pre-injury status, but the reduced pain creates the impression that full recovery is complete. Research consistently identifies the 2–4 week post-return period as the highest recurrence risk window for muscle strains and ligament sprains — the athlete returns to full training, the protective pain signal that previously modulated loading is reduced, and the tissue is re-exposed to maximal loading before full structural recovery is achieved. Preventing recurrence: continue the injury-specific strength and mobility work from the rehabilitation phase as a permanent part of the training program (the weakness or movement restriction that contributed to the original injury will return if the rehabilitation exercises are discontinued at return to sport); reduce session intensity by 20–30% for the first 2 weeks of full training resumption; and maintain heightened attention to pain signals at the injury site during this period — any reproduction of the original pain pattern should prompt immediate load reduction and reassessment rather than the push-through approach that produced the original injury. From NATA guidelines on injury recurrence prevention, athletes who complete formal rehabilitation — including sport-specific movement preparation and return-to-sport testing — have significantly lower recurrence rates than those who return based on subjective pain resolution alone.
Psychological Preparation: The Mental Approach to Pain and Injury
Beyond the physical rehabilitation that acute sharp pain injury requires, the psychological preparation for managing pain, uncertainty, and the rehabilitation process determines how effectively and quickly athletes return to full training. The athlete who approaches injury with catastrophizing (this injury will end my training permanently), helplessness (there is nothing I can do to influence recovery speed), or avoidance (refusing to move the injured area at all because any discomfort feels threatening) consistently recovers more slowly than the athlete who approaches injury with acceptance, active engagement in rehabilitation, and realistic optimism about recovery timeline. The evidence-based psychological approaches for injury recovery: goal setting (establishing specific, measurable, achievable, relevant, and time-bound rehabilitation goals provides the progress markers that maintain motivation across the often-frustrating rehabilitation timeline); imagery (mental rehearsal of performing the movements that injury currently prevents, maintaining the neuromuscular patterns that injury rehabilitation must restore when physical loading becomes possible); attentional focus training (directing attention to movement quality and proprioceptive feedback rather than to pain levels during rehabilitation exercises reduces pain catastrophizing and improves movement re-learning); and social support (maintaining connection with training partners and coaches during injury rehabilitation reduces the social isolation that injury produces and maintains the athletic identity that injury can threaten). The return-to-training decision is both a physical and psychological readiness assessment — athletes who are physically capable of returning to training but psychologically unprepared (significant residual fear of re-injury, loss of confidence in the injured body part’s reliability) benefit from graduated exposure to increasingly demanding movements with a physiotherapist present, building the psychological confidence alongside the physical capacity that full athletic performance requires.
Apply these principles daily.

When to See a Doctor: Red Flags, Serious Conditions, and FAQs
Most sharp exercise pain episodes represent soft tissue injuries manageable with self-care and physiotherapy — but a subset require urgent medical evaluation for potentially serious pathology that self-management is inappropriate for. Knowing which signs and symptoms mandate immediate medical attention prevents the delayed treatment of genuinely serious conditions.
Absolute Red Flags: Seek Emergency Medical Care Immediately
The following presentations during or after exercise require emergency medical response — calling emergency services or proceeding immediately to the nearest emergency department: chest pain of any quality during exercise (sharp, crushing, pressure, or burning) — until proven otherwise, treat as potential cardiac event; severe shortness of breath disproportionate to exercise intensity, particularly with chest pain, dizziness, or syncope; sharp pain in the chest radiating to the left arm, jaw, or back; sudden severe headache during exercise (described as “the worst headache of my life” — the presentation of subarachnoid hemorrhage); significant joint deformity after injury (bone visible through skin, joint clearly dislocated from its normal position); complete inability to bear weight on an injured lower limb with severe pain; and loss of sensation or movement in a limb following injury. These presentations require emergency evaluation regardless of the athlete’s belief that the pain is exercise-related — cardiac events, intracranial hemorrhage, and serious structural injuries have occurred during exercise in athletes of all fitness levels and ages, and the delay of medical evaluation in these scenarios can be fatal or produce permanent disability.
Urgent Medical Referral: Within 24–48 Hours
The following sharp exercise pain presentations warrant urgent (not emergency) medical evaluation — seeing a physician or sports medicine specialist within 24–48 hours rather than attempting self-management: significant joint swelling appearing within 2 hours of injury (hemarthrosis — blood in the joint — indicating significant ligamentous or cartilage injury, most critically ACL tear); audible pop or crack at the moment of injury in a major joint (knee, ankle, shoulder) followed by significant functional limitation; any sharp pain in a long bone (tibia, femur, humerus) that worsens progressively with activity over days to weeks (bone stress fracture pattern); sharp pain with neurological symptoms (numbness, tingling, or weakness in a dermatomal or peripheral nerve distribution — indicating nerve compression or injury); shoulder or hip dislocation (the joint locked in an abnormal position with severe pain and inability to return to normal position through self-reduction attempts); and any acute injury that does not begin to improve within 5–7 days of appropriate self-management.
Frequently Asked Questions About Sharp Exercise Pain
Is it okay to train through sharp pain if I tape or brace the area? No — taping and bracing reduce the pain signal without addressing the underlying tissue damage; training through sharp pain with external support risks further tissue damage because the protective pain signal that would normally limit loading is suppressed. Use taping and bracing to support healing tissue during recovery, not to enable continued high-intensity training through pain. How do I know if I need an X-ray after a sharp exercise pain episode? The Ottawa Knee Rules (for knee pain) and Ottawa Ankle Rules (for ankle pain) — validated clinical tools — provide the criteria for when imaging is needed. Generally: ability to bear weight on the injured limb, absence of bony tenderness at specific anatomical points, and absence of significant swelling within 2 hours of injury suggest imaging is not immediately necessary. When in doubt, seek medical assessment. Can sharp exercise pain be prevented with supplements? No supplement prevents acute mechanical injury. Collagen supplementation (5–15g before training, with vitamin C) has emerging evidence for supporting tendon and ligament health that may reduce chronic injury risk over time — but acute tissue failure from mechanical overload is not preventable through nutritional supplementation. Why does sharp pain sometimes disappear during exercise but return afterward? The adrenaline and endorphin response to intense exercise temporarily raises the pain threshold — masking pain during exercise that returns when the adrenergic response subsides. This mechanism is why athletes sometimes report not feeling their injury until after the game or training session. It does not indicate that continuing to train after the pain appears is safe — it indicates that the pain-masking response of intense exercise has temporarily obscured genuine tissue damage. How long after sharp exercise pain can I return to sport? Return depends on injury type, severity, and sport demands — from 3–7 days for Grade 1 muscle strains in low-impact sports to 6–12 months for ACL reconstruction in cutting and pivoting sports. Consult a physiotherapist or sports medicine physician for a rehabilitation timeline specific to the injury and sport. Should I use heat or ice on a sharp exercise pain injury? In the first 72 hours: neither is strongly recommended by current evidence; if pain management is needed, brief ice application (15 minutes maximum) is acceptable. After 72 hours: heat can be applied to encourage blood flow and tissue extensibility before rehabilitation exercises — but should not be applied to acutely swollen tissue.
Building Long-Term Injury Resilience: The Sustainable Training Approach
Injury resilience — the capacity to sustain high training loads across years without acute sharp pain episodes or significant injury downtime — is built through consistent application of the prevention principles in this section, combined with the patience to progress loads gradually enough that tissue adaptation keeps pace with loading demand. The athletes with the best long-term injury records are not those who train least intensely — they are those who apply the most systematic approach to load progression, recovery, and movement quality that prevents the tissue overload that training at any intensity eventually produces without appropriate management. The long-term injury resilience framework: establish a baseline training load at which injury risk is low and performance is improving, and hold this load for 8–12 weeks before beginning gradual increase; never exceed 10–15% week-to-week load increase; schedule deload weeks every 4–6 weeks regardless of subjective readiness (planned recovery prevents the accumulated fatigue that unplanned injury-enforced recovery interrupts); include 2–3 sessions per week of injury prevention exercises (hamstring curls, hip abduction, rotator cuff work, single-leg balance) as permanent training program components rather than temporary rehabilitation additions; address movement restrictions proactively through regular mobility work before they become pain-producing under load; and schedule quarterly check-ins with a physiotherapist or sports medicine professional for movement assessment and early identification of developing tissue stress before it produces acute injury. This systematic approach converts injury prevention from a reactive response to acute events into the proactive training program component that maintains the training continuity that long-term athletic development requires. The sharp exercise pain episode is the body’s most urgent communication that the current training approach requires modification — respond to it with the evidence-based protocol in this article, and use it as the prompt to implement the prevention practices that reduce the probability of the next episode.
The athlete who reads this article and implements its guidance — the pain classification framework, the acute response protocol, the prevention practices, and the rehabilitation principles — possesses the exercise pain management knowledge that converts sharp exercise pain from a feared, unpredictable training disruptor into a manageable, informative body signal that guides evidence-based training decisions. Sharp exercise pain is not the enemy of athletic development — it is one of the body’s most reliable communication mechanisms, telling the athlete precisely what tissue is being overloaded and what adaptation the training program currently lacks. Listen to it, respond appropriately, address the underlying cause, and return to training with the modifications that prevent recurrence. This is the complete cycle of exercise pain management that sustains the long, productive athletic career that consistent, injury-informed training produces. The sharp pain that stops a workout is the teacher, not the terminator — approach it as such, extract the information it provides, and use that information to train smarter, progress more consistently, and build the injury-resilient athletic body that years of evidence-based training and intelligent pain management develop. The practical knowledge in this article — from the five-criteria pain classification framework through the PEACE and LOVE acute management protocol, the periodization and proprioception-based prevention practices, and the evidence-based return-to-sport criteria — provides the complete toolkit for managing sharp exercise pain at every stage: recognizing it accurately, responding appropriately in the moment, recovering systematically, and preventing recurrence through structural training program modifications. Implement these principles not reactively when pain occurs, but proactively as the permanent foundation of a training program that supports decades of athletic development without the injury interruptions that uninformed training approaches inevitably produce. The investment in understanding sharp exercise pain — reading this article, implementing the prevention practices, and responding to pain signals with evidence rather than bravado — returns compounding dividends across every training year: more sessions completed, more progressive overload achieved, more adaptation accumulated, and the long athletic career that training smart as well as training hard ultimately produces. Your body communicates through pain because it has no other language for urgency — learn to listen, learn to respond, and let that communication guide you toward the most productive, safest, and most sustainable athletic development path available to you.




