Lower Back Pain From Exercise: Causes, Fixes, and Prevention Tips
This article is for general educational purposes only and does not constitute medical or professional fitness advice.
Stop exercise and consult a licensed healthcare provider if you experience sharp, worsening, or persistent pain.
Lower back pain is among the most prevalent musculoskeletal complaints worldwide — and exercise is a common trigger for both its onset and its recurrence.
Understanding why exercise-related lower back pain happens — and what to do when it does — can help you train more safely and manage symptoms more effectively.
Important: This guide covers general exercise-related lower back discomfort. If you experience severe pain, pain with neurological symptoms (numbness, tingling, weakness in the legs), or pain following trauma — please seek medical evaluation before attempting any exercise modification.
Common Exercise-Related Causes of Lower Back Pain
The Most Frequent Culprits
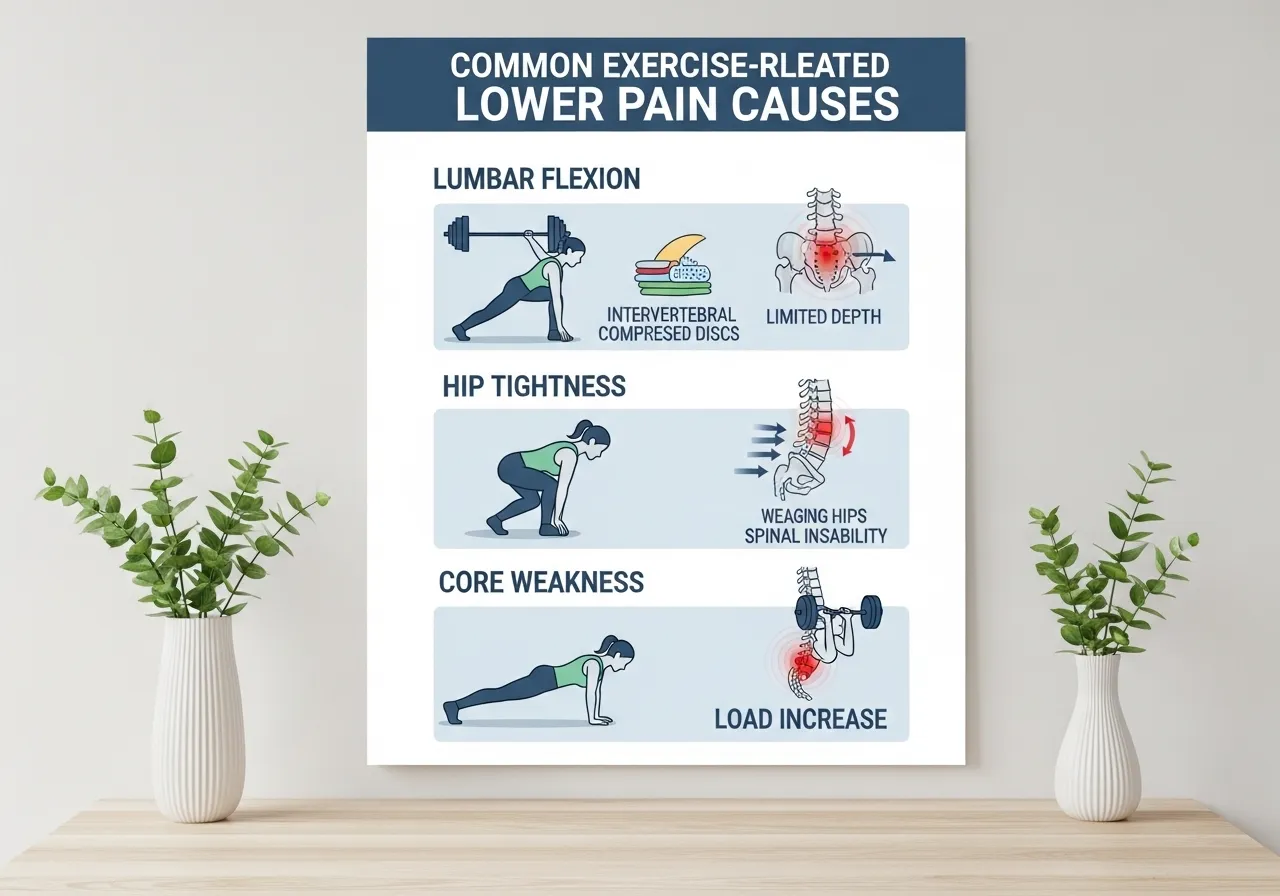
Lower back pain during or after exercise most commonly results from:
| Cause | Common Scenario | Primary Structure Affected |
|---|---|---|
| Lumbar flexion under load | Rounding the lower back during deadlifts or squats | Intervertebral discs (L4–L5, L5–S1) |
| Hip flexor tightness | Excessive anterior pelvic tilt during exercise | Lumbar extensors, facet joints |
| Weak core stability | Spine unable to maintain position under load | Spinal musculature, discs |
| Rapid volume increase | Too much new stress before adequate adaptation | Posterior spinal muscles |
| Poor hip mobility | Hip compensates by shifting load to the lumbar spine | Lumbar discs and joints |
Flexion-Intolerant vs Extension-Intolerant Pain
Lower back pain patterns often fall into one of two categories — and the distinction matters because the appropriate exercise modifications differ:
- Flexion-intolerant (pain worsened by bending forward, sitting, or rounding the spine): often associated with disc involvement — extension-based movements may feel relieving
- Extension-intolerant (pain worsened by arching backward or standing for long periods): often associated with facet joints or spinal stenosis — flexion-based positions may feel relieving
A physical therapist can perform a more precise assessment to identify your pattern and guide appropriate exercise selection.
Immediate Management: What to Do When Lower Back Pain Occurs
The Evidence on Rest
Prolonged bed rest (complete inactivity for more than 1–2 days) is no longer recommended for most non-specific lower back pain — current clinical guidelines consistently support staying gently active within a pain-tolerable range as preferable to extended rest.
However, this does not mean continuing the activity that caused the pain at the same intensity.
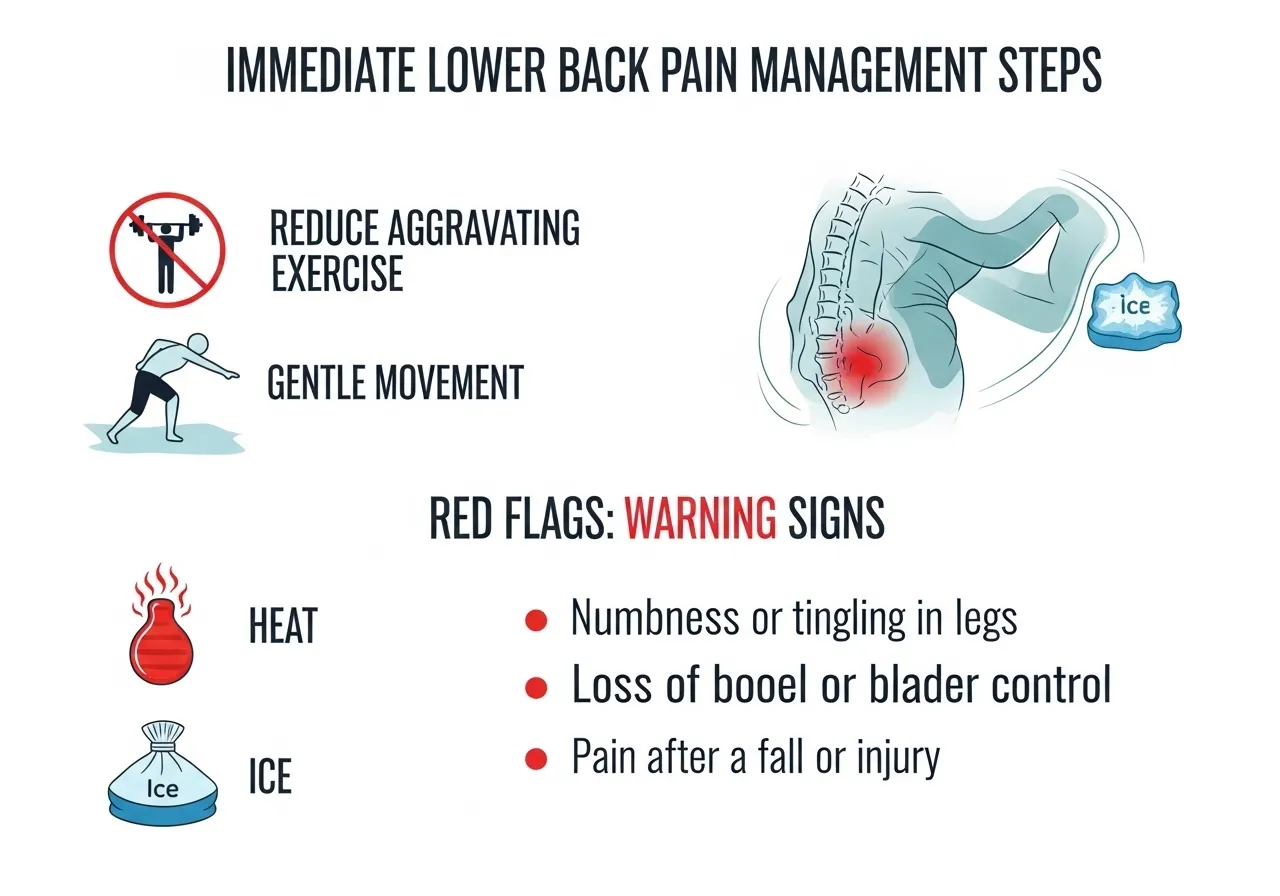
Immediate Steps
🔵 Maintain gentle movement — walking is often well-tolerated and may support recovery
🔵 Apply heat or ice — both can provide temporary symptom relief for some individuals; personal preference often determines which is more helpful
🔵 Avoid prolonged sitting or standing — position changes every 20–30 minutes may reduce cumulative spinal loading
When to Seek Medical Evaluation
• Numbness, tingling, or weakness in one or both legs (possible nerve involvement)
• Bladder or bowel dysfunction accompanying back pain (requires emergency evaluation)
• Pain following a fall, impact, or lifting incident with high force
• Fever, unexplained weight loss, or night sweats alongside back pain
• Symptoms that progressively worsen over 2–3 weeks despite rest
Exercise Modifications and Rehabilitation Approaches
Generally Well-Tolerated Starting Points
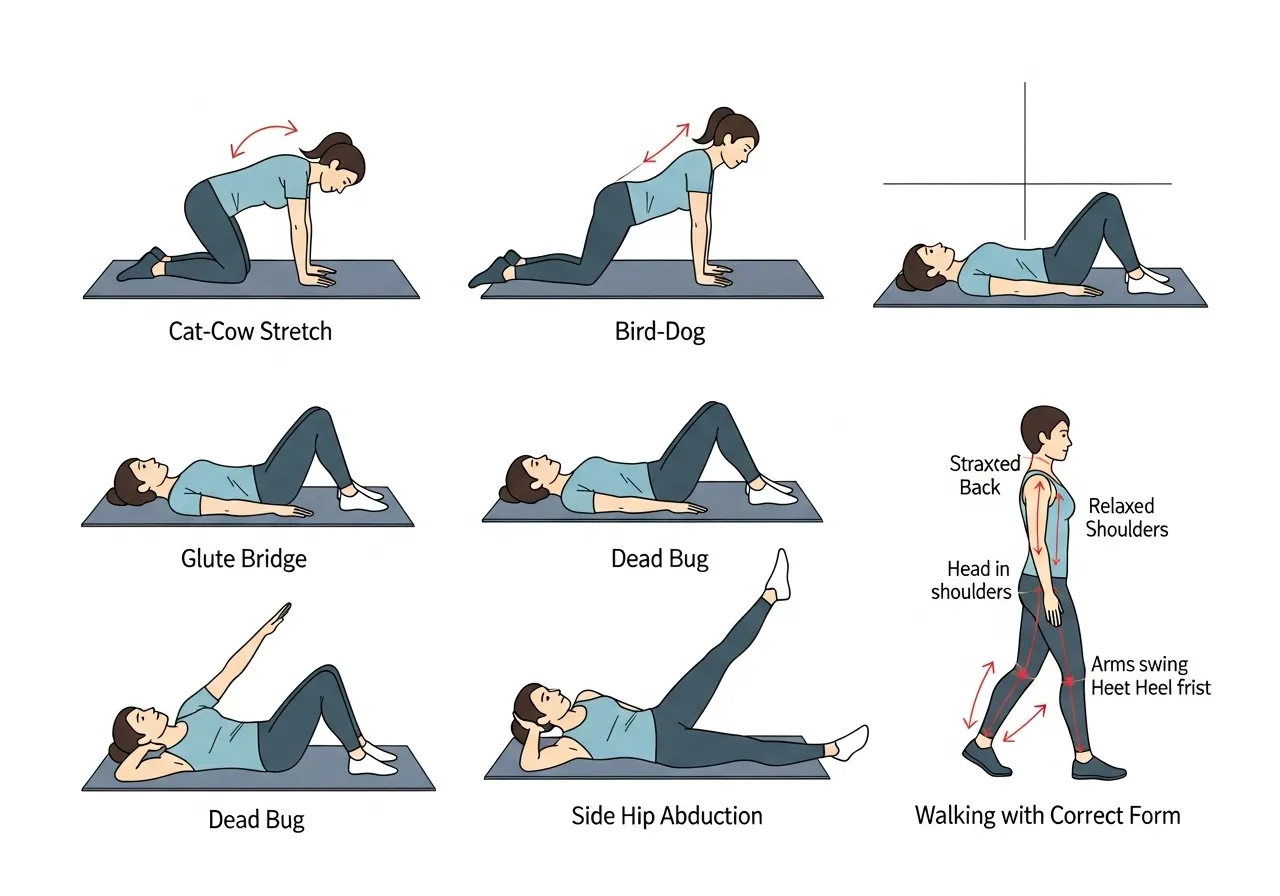
For most cases of non-specific exercise-related lower back pain, the following movements are often well-tolerated and may support recovery — but individual responses vary considerably:
✅ Cat-cow stretch — controlled spinal flexion-extension in an unloaded position
✅ Bird-dog — anti-extension core exercise; builds lumbar stability without spinal loading
✅ Glute bridge — activates glutes and posterior chain without significant spinal compression
✅ Side-lying hip abduction — addresses hip weakness without lumbar loading
✅ Dead bug — builds deep core stability in a supine (lying on the back) position
Movements to Approach Cautiously (Until Evaluated)
⚠️ Sit-ups and crunches — significant lumbar flexion under load
⚠️ Leg press with deep hip flexion — can increase posterior pelvic tilt under load
⚠️ Running and high-impact activities — until acute symptoms have meaningfully reduced
Core Stability vs Core Strength: An Important Distinction
During the early rehabilitation phase, core stability (the ability to prevent unwanted spinal movement) is generally prioritized over core strength (the ability to produce large forces).
This is why anti-movement exercises (plank, bird-dog, dead bug, Pallof press) are typically recommended before returning to heavy loaded movements — they develop the positional control that protects the spine during subsequent strength training.
Long-Term Prevention: Keeping Lower Back Pain From Recurring
Address the Root Cause, Not Just the Symptom
Lower back pain often recurs because the underlying factors that caused the initial episode are never fully addressed.
The most common addressable contributors include:
1 — Hip Flexor and Thoracic Mobility
Tight hip flexors create anterior pelvic tilt (the pelvis tipping forward, increasing lumbar extension), which increases compressive loading on the lumbar facet joints during exercise and daily activity.
Daily hip flexor stretching (kneeling lunge stretch, 30 sec × 3 each side) and thoracic mobility work (foam roller extension over mid-back, 2 min daily) may meaningfully reduce this contributing factor over several weeks.
2 — Glute Activation and Posterior Chain Strength
Weak or inhibited glutes (a common consequence of prolonged sitting) force the lumbar erectors to compensate during hip-dominant movements — increasing the load on spinal structures relative to the intended target muscles.
Exercises that specifically target glute activation — hip thrusts, Romanian deadlifts, single-leg glute bridges — may reduce lumbar compensation patterns over time.
3 — Consistent Core Stability Training
Maintaining a baseline of core stability training long-term — not only during acute episodes — may reduce recurrence risk. Anti-extension (plank), anti-rotation (Pallof press), and anti-lateral flexion (suitcase carry) exercises each train different aspects of spinal stability.
4 — Load Management Principles
Increasing training load (weight, volume, intensity) by no more than approximately 10% per week, allowing adequate recovery between sessions, and including deload weeks every 4–8 weeks applies to lower back pain prevention as much as to general injury prevention.
- Lower back pain during exercise most commonly results from lumbar flexion under load, hip tightness, or rapid load increases
- Staying gently active (walking, light mobility work) is generally preferred over extended bed rest for most non-specific cases
- Core stability exercises (bird-dog, dead bug, plank) are a well-supported starting point during rehabilitation
- Neurological symptoms (leg numbness, weakness, or bowel/bladder changes) require prompt medical evaluation
- Addressing hip flexor tightness, glute weakness, and load management may help reduce recurrence

Frequently Asked Questions About Lower Back Pain and Exercise
Q: Should I stop exercising when my lower back hurts?
Not necessarily — but modifying rather than stopping is generally recommended for most non-specific lower back discomfort.
Completely stopping exercise may actually slow recovery by reducing blood flow, weakening supporting musculature, and disrupting the behavioral pattern of regular movement.
The key is identifying which specific exercises are provocative and avoiding those while maintaining activity through pain-tolerable alternatives.
Q: Is deadlifting bad for the lower back?
Performed with appropriate mechanics and progressive loading, the deadlift is not inherently dangerous for the lower back — and may actually strengthen the posterior chain structures that support spinal health over time.
The risk arises when the lower back is rounded under load, when weight exceeds current technique capacity, or when load is increased faster than the spine can adapt.
If you have experienced lower back pain during deadlifting, working with a certified trainer or physical therapist to assess your form before continuing under load may be worthwhile.
Q: How do I know if it’s a disc problem or muscle strain?
Self-diagnosis is not reliable for this distinction — both can produce similar pain experiences. However, some general patterns:
- Disc-related pain often refers down the leg (sciatica — pain along the sciatic nerve pathway) and may worsen with prolonged sitting
- Muscle strain is typically localized to the back, often worse with movement and better with rest, and tends to improve within days to weeks
If pain refers down the leg, is accompanied by numbness or tingling, or does not improve within 2–3 weeks of conservative management, an evaluation by a sports medicine physician or physical therapist is strongly recommended.