How to Prevent and Treat Runner’s Knee


1. What Is Runner’s Knee? Causes, Anatomy, and Who Gets It
Runner’s knee — clinically termed patellofemoral pain syndrome (PFPS) — is the most common running injury and one of the most prevalent musculoskeletal complaints in active adults, accounting for approximately 25% of all running-related injuries and 16–25% of all knee pain presentations in sports medicine clinics. Despite its name, runner’s knee affects cyclists, hikers, skiers, football players, and anyone who subjects the knee to repeated flexion-extension loading — running is simply the most common context in which the cumulative loading that produces patellofemoral pain occurs. I experienced runner’s knee at mile 8 of what was supposed to be a 15-mile long run — the gradual onset of diffuse anterior knee pain that forced my pace to slow, then my run to stop, and finally kept me off running trails for six frustrating weeks before I understood what was happening and how to address it. This article provides the complete patellofemoral pain guide I wish I had found in those six weeks.
The Patellofemoral Joint: Anatomy and Function
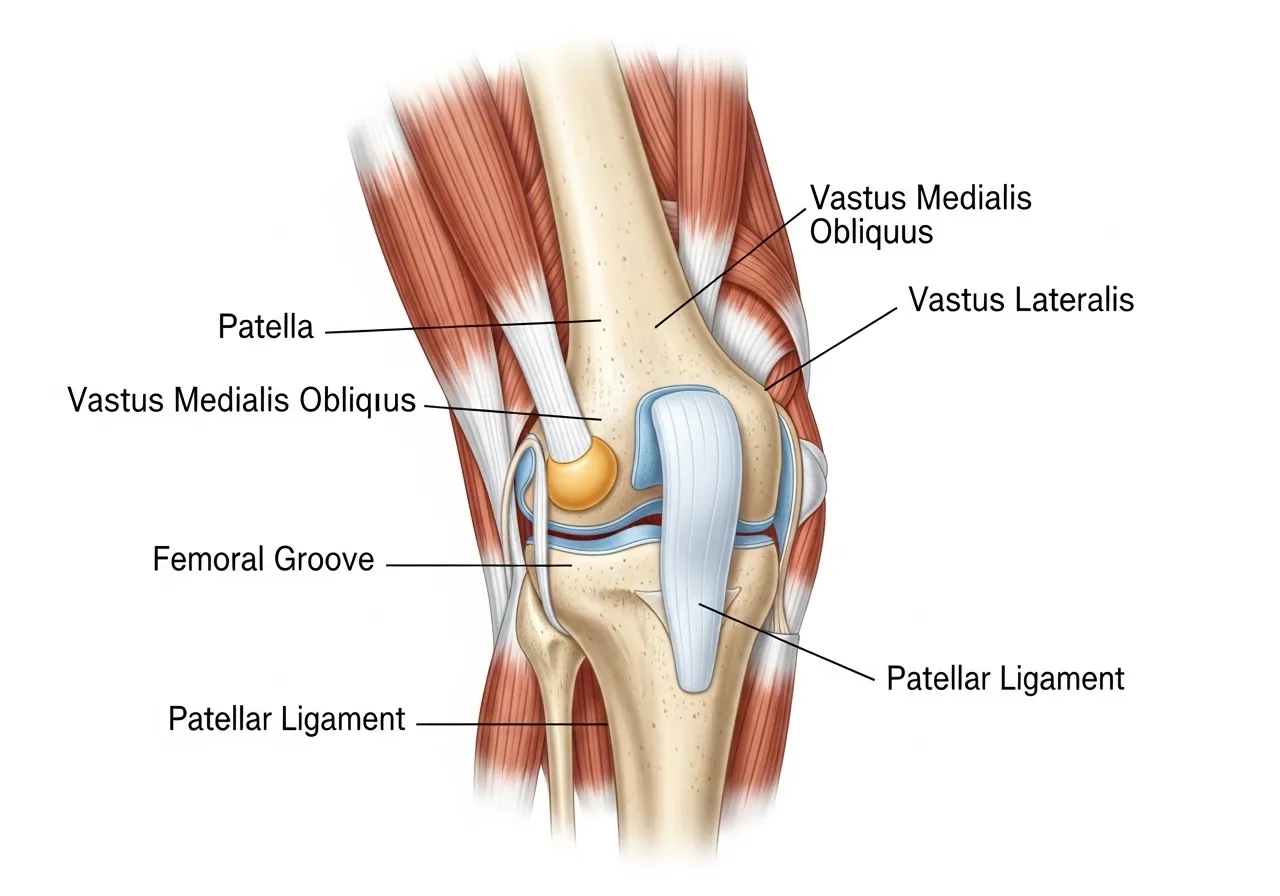
The patellofemoral joint — the articulation between the patella (kneecap) and the femoral trochlea (the groove on the front of the femur in which the patella tracks during knee flexion) — is a sesamoid joint whose primary function is to increase the mechanical advantage of the quadricep muscle group for knee extension. The patella sits within the quadricep tendon and translates the pulling force of the four quadricep muscles (vastus medialis, vastus lateralis, vastus intermedius, rectus femoris) into the patellar tendon that attaches to the tibial tuberosity — the bony prominence below the kneecap where the extension force is ultimately applied. During walking, the patellofemoral joint experiences forces of approximately 0.5 times body weight; during stair climbing, this increases to 3–4 times body weight; during running, patellofemoral joint reaction forces reach 7–12 times body weight depending on running speed, stride mechanics, and the specific phase of the gait cycle. These forces are distributed across the articular cartilage that covers the posterior surface of the patella and the femoral trochlea — cartilage that is approximately 4–5mm thick in the patella, the thickest in the body, reflecting the substantial forces this joint routinely experiences. From British Journal of Sports Medicine research on patellofemoral biomechanics, the cartilage health of the patellofemoral joint depends on appropriate load distribution across the joint surface — when the patella tracks laterally (toward the outside of the knee) rather than centrally in the femoral groove, the contact area decreases and the stress per unit area increases, eventually exceeding the cartilage’s tolerance for repeated loading.
The Causes of Runner’s Knee: Why the Patella Tracks Incorrectly
Patellofemoral pain syndrome is not a single-cause condition — it is the final common pathway of multiple biomechanical, anatomical, and training-related factors that produce excessive or maldistributed stress on the patellofemoral joint. The most well-established contributing factors: quadricep muscle imbalance (the vastus medialis oblique — VMO, the teardrop-shaped muscle on the inner side of the thigh — provides the medial pull that keeps the patella centered in the femoral groove; weakness or delayed activation of the VMO relative to the vastus lateralis allows the lateral quadricep force to dominate, pulling the patella laterally and increasing lateral facet contact stress); hip abductor and external rotator weakness (the gluteus medius, minimus, and external rotators control femoral adduction and internal rotation during single-leg stance — weakness allows the femur to drop inward during running, effectively moving the femoral trochlea medially relative to the fixed patella, increasing lateral patellofemoral stress without any change in the patella’s tracking pattern); foot pronation and subtalar mechanics (excessive foot pronation during running produces tibial internal rotation that is transmitted to the femur, contributing to the dynamic knee valgus that increases patellofemoral stress — the foot-to-knee kinetic chain connection means that foot mechanics affect knee joint loading); and training load errors (sudden increases in running volume, introduction of hill running, starting speed training, or changing footwear all constitute the training load changes that exceed the patellofemoral joint’s adaptation capacity and initiate the pain cycle).
Who Gets Runner’s Knee and Why
Runner’s knee affects women at approximately 2:1 frequency compared to men — a disparity attributed to several anatomical and biomechanical factors. The Q-angle (the angle between the line from the anterior superior iliac spine to the patella and the line from the patella to the tibial tuberosity) is typically greater in women due to the wider pelvis of female anatomy — a larger Q-angle increases the lateral vector force on the patella during quadricep contraction, predisposing to lateral tracking and increased patellofemoral stress. Women also show greater tendency toward dynamic knee valgus during running and jumping (the femur dropping inward during single-leg loading), which is associated with hip abductor and external rotator weakness that is more prevalent in female runners. Beginning runners are particularly susceptible — the combination of unconditioned hip and quadricep musculature, often incorrect biomechanics developed from walking rather than running-specific movement patterns, and the rapid mileage increases that beginner enthusiasm drives creates the perfect conditions for patellofemoral overload. Masters runners (40+) face increasing risk as the cartilage remodeling capacity of the patellofemoral joint decreases with age — the same training loads that were tolerable at 30 may exceed the aging cartilage’s adaptive capacity at 50, particularly without the strength training that maintains the muscular protection that cartilage depends on. Athletes returning from lower limb injuries (ankle sprains, hamstring strains, calf injuries) are at elevated risk because the compensatory movement patterns adopted during the primary injury recovery period can alter hip and knee loading mechanics in ways that produce secondary patellofemoral overload.
The Pain Mechanism: Why Runner’s Knee Hurts Where It Does
The pain of patellofemoral pain syndrome originates from the subchondral bone beneath the articular cartilage of the patella and femoral trochlea, the synovial membrane of the patellofemoral joint, and the retinacular (connective tissue) structures that surround the kneecap — not typically from the articular cartilage itself, which is aneural (containing no pain fibers). This explains the characteristic diffuse, poorly localized anterior knee pain of PFPS — the pain arises from the innervated structures surrounding the joint rather than from a specific anatomical point. The pain is characteristically provoked by activities that increase patellofemoral joint reaction force: prolonged sitting with the knee flexed (the theatre sign — pain after sitting in cinema, car, or desk for 30+ minutes, relieved by standing and walking); descending stairs (the highest single-leg patellofemoral loading activity in daily life); squatting; running particularly on downhill grades; and kneeling. The pain is typically absent at rest (distinguishing it from the rest pain of inflammatory arthritis) and develops gradually during provocative activities rather than beginning suddenly at the onset of activity. Understanding this pain mechanism — the subchondral bone and retinacular tissue responding to excessive mechanical loading of the patellofemoral joint — guides the treatment approach: reduce the patellofemoral joint stress through load modification, biomechanical correction, and strengthening the muscles that distribute patellofemoral forces optimally.
The Psychological Impact of Runner’s Knee and Managing Training Identity
For dedicated runners, a runner’s knee diagnosis carries psychological weight beyond the physical pain — the identity disruption of being unable to run, the anxiety about permanent damage, and the frustration of watching training gains erode during the rehabilitation period collectively produce the psychological burden that accompanies any significant athletic injury. Acknowledging this psychological dimension and managing it proactively is as important as the physical rehabilitation for complete recovery. The training identity maintenance strategy: reframe the rehabilitation period as training for the structural qualities (hip strength, VMO activation, gait mechanics) that running cannot develop alone — the runner who emerges from PFPS rehabilitation is biomechanically stronger, more durable, and better protected against future injury than the runner who entered it. This reframe is not merely positive spin — it is physiologically accurate. The hip strength deficits and gait mechanics errors that PFPS reveals were present before the injury; the rehabilitation program addresses them definitively for the first time. The post-rehabilitation runner genuinely is more resilient than the pre-injury version. Maintaining cardiovascular fitness through pool running, swimming, and cycling during the land-running restriction preserves the aerobic base that returning to running depends on — pool running (running in the deep end of a pool with a flotation belt) produces cardiovascular training nearly identical to land running without the patellofemoral loading, making it the highest-value cross-training activity for injured runners. Setting rehabilitation milestones — the first pain-free 5-minute run, the first pain-free 10-minute run, the first continuous 20-minute run — provides the progress markers that maintain motivation ac The comprehensive management of runner’s knee — from accurate diagnosis through systematic rehabilitation to permanent prevention — is fully achievable by any motivated runner willing to invest the 6–12 weeks of consistent effort that the evidence-based program described in this article requires. The patellofemoral joint that is producing anterior knee pain today can become the structurally sound, well-supported joint that carries a runner through decades of training and racing — but only if the biomechanical vulnerabilities that PFPS reveals are addressed through the targeted strengthening, gait modification, and load management that conservative rehabilitation provides. The tools are in this article. The timeline is realistic. The outcomes for runners who implement the full rehabilitation program are consistently positive — pain resolution, return to full training, performance improvement, and the injury resilience that prevents recurrence. Begin the hip strengthening exercises today, modify the training load immediately, and commit to the 8-week return-to-running protocol when the criteria for beginning it are met. The pain-free running that awaits on the other side of this rehabilitation journey is worth every step of the structured, evidence-based process that gets you there. Runner’s knee does not have to define your running story — it can be the chapter that makes the rest of the story possible. The science of patellofemoral pain syndrome has advanced considerably in the past decade — the understanding of hip weakness as a primary driver has shifted rehabilitation focus from isolated quadricep training toward the comprehensive hip-and-knee approach that produces superior outcomes. The runners who benefit most from this updated understanding are those who receive comprehensive rehabilitation from physiotherapists familiar with current PFPS research, rather than the outdated advice of simply strengthening the VMO with isolated exercises that older protocols emphasized. Seek a physiotherapist with experience in running injury rehabilitation — specifically one who performs gait analysis, assesses hip strength quantitatively, and provides a progressive exercise program rather than generic knee exercises. The quality of the rehabilitation guidance significantly determines the recovery timeline and the completeness of the biomechanical correction that prevents recurrence. A 6-session course of physiotherapy — assessment, exercise prescription, gait retraining cues, and progressive monitoring — is one of the highest-value medical investments a runner with PFPS can make, producing the personalized rehabilitation plan that this article’s general guidance cannot replace. The information in this article provides the framework; the physiotherapist provides the individualization. Together, they give the runner with patellofemoral pain syndrome the best possible chance of rapid, complete, and lasting recovery — returning to the running that sustains their health, their competitive goals, and the daily practice that running-identity athletes treasure as one of the most important elements of their lives. Run smart, run strong, and run free from knee pain. Be patient. Stay committed. Succeed.
2. Symptoms and Diagnosis: How to Know If You Have Runner’s Knee
Accurate diagnosis of patellofemoral pain syndrome is essential for appropriate management — several other knee conditions (iliotibial band syndrome, patellar tendinopathy, medial plica syndrome, fat pad impingement) produce anterior or peripatellar knee pain that superficially resembles PFPS but requires different treatment. This section provides the symptom profile, clinical tests, and differential diagnosis guidance that allows accurate self-identification and informs the decision about when professional assessment is warranted.
The Classic PFPS Symptom Profile
Runner’s knee presents with a characteristic symptom cluster that distinguishes it from other knee pain conditions. Location: diffuse, poorly localized pain around, under, or behind the kneecap — the athlete typically cannot point to a single specific pain point but gestures around the entire front of the knee. This diffuse location contrasts with the specific single-point tenderness of patellar tendinopathy (pain at the inferior patellar pole) and the lateral knee pain of iliotibial band syndrome (maximum pain at the lateral femoral condyle, approximately 2cm above the joint line). Provocative activities: pain with prolonged sitting (positive theatre sign), descending stairs, squatting, and running — particularly on downhill grades. The downhill running provocation is highly characteristic of PFPS — the increased knee flexion angle and quadricep eccentric demand of downhill running produces the greatest patellofemoral contact forces and is the running condition that most reliably reproduces patellofemoral pain. Onset pattern: typically gradual onset during or after running rather than sudden acute onset — the pain often begins as a mild ache that worsens with continued activity, improves with rest, and returns at the same point in subsequent runs. A common pattern: the runner is pain-free for the first 15–20 minutes of the run, develops increasing anterior knee pain that forces pace reduction between 20–40 minutes, and eventually cannot continue at 40–60 minutes despite warming up normally at the start. Swelling: mild joint effusion (excess fluid in the knee joint) may be present after high-load activities, but significant swelling is uncommon in PFPS — significant swelling suggests a more serious intra-articular pathology requiring medical assessment.
Self-Assessment Tests and When to See a Professional
Several clinical tests can be self-administered to support the diagnosis of PFPS, though professional assessment remains the gold standard. The Clarke’s test: sit with the knee extended, place the web of the hand just above the patella and apply mild downward and lateral pressure, then contract the quadricep (try to straighten the knee against the hand pressure). Pain reproduction with this maneuver suggests patellofemoral involvement, though the test has modest sensitivity and specificity and should be interpreted alongside the symptom history. The step-down test: stand on one leg on a step and slowly lower the other leg toward the floor, observing for knee pain reproduction and knee valgus collapse (the knee moving inward during the single-leg squat — a positive finding for hip abductor weakness). The theatre sign self-assessment: sit with the knee at approximately 90 degrees for 20–30 minutes (as in a cinema or car) — pain developing or increasing during this sustained flexion is characteristic of PFPS. Seek professional assessment when: the knee pain is severe or does not respond to 2 weeks of load modification and the exercises in Section 4; significant swelling is present; the knee locks, gives way, or produces mechanical symptoms (clicking or catching associated with pain); or the pain began after a specific traumatic incident rather than gradual overuse onset. From JOSPT clinical guidelines for patellofemoral pain, physiotherapist assessment provides the clinical examination, movement analysis, and differential diagnosis that self-assessment cannot replicate — identifying the specific contributing factors (VMO weakness, hip weakness, biomechanical errors, foot mechanics) that should guide the rehabilitation program.
Differential Diagnosis: Ruling Out Other Knee Conditions
The most important conditions to distinguish from PFPS in runners: iliotibial band syndrome (ITBS) produces lateral knee pain (outer side of the knee, at or above the lateral joint line) that is reproduced by the Noble compression test (direct pressure on the lateral femoral condyle at 30 degrees of knee flexion) — ITBS pain is precisely lateral rather than anterior and diffuse. Patellar tendinopathy produces localized pain at the inferior pole of the patella (the bottom tip of the kneecap) or along the patellar tendon — the pain is precisely located, reproduced by direct palpation of the tendon, and is worst with jumping and impact activities rather than sustained knee flexion. Medial plica syndrome produces medial knee pain from the inflamed medial synovial fold — distinguishable from PFPS by its medial rather than anterior location and the snapping or catching sensation that plica irritation sometimes produces. Fat pad impingement (Hoffa’s syndrome) produces pain inferior to the patella and the patellar tendon — reproduced by extending the knee fully (compressing the fat pad between the patella and femoral condyle) and by direct pressure on the fat pad. Patellar stress fracture — rare but important — produces point tenderness on the patella itself, pain with resisted knee extension, and often has an antecedent history of sudden load increase; it requires imaging for diagnosis. If the symptom pattern does not clearly match PFPS or if there is diagnostic uncertainty, professional assessment with imaging as indicated (X-ray to exclude osseous pathology, MRI for soft tissue and cartilage assessment) provides the definitive diagnosis that guides appropriate management.
ross the weeks of gradual improvement that PFPS rehabilitation requires.
Nutrition for Patellofemoral Cartilage Health
The articular cartilage of the patellofemoral joint — the tissue that excessive loading damages in PFPS — is avascular (without direct blood supply) and depends on diffusion of nutrients from the synovial fluid for its metabolic needs. This avascular nature makes cartilage remodeling and repair slower than vascular tissues, and nutritional support for cartilage health is an important adjunct to mechanical load management and rehabilitation exercise. The evidence-based nutritional interventions for joint cartilage health: collagen supplementation (10–15g of hydrolyzed collagen or gelatin consumed 30–60 minutes before exercise, with 200mg of vitamin C, stimulates periarticular collagen synthesis in the periods of elevated blood amino acid levels that follow exercise — providing the building blocks for cartilage matrix maintenance); omega-3 fatty acids (2–3g of EPA and DHA daily from fish oil reduces the synovial inflammation that PFPS produces, potentially reducing pain and the secondary cartilage effects of chronic synovial inflammation); vitamin D (adequate vitamin D status is associated with reduced musculoskeletal pain and better muscle function — athletes with vitamin D deficiency show impaired quadricep and hip muscle function that contributes to biomechanical PFPS risk factors); and adequate total protein intake (1.6–2.2g/kg body weight provides the amino acid substrate for the musculotendinous and articular tissue remodeling that rehabilitation requires). These nutritional strategies do not replace the mechanical interventions of load modification and exercise rehabilitation — but they support the biological processes that rehabilitation depends on, potentially accelerating the recovery timeline and improving the tissue quality of the remodeled structures.
Understanding the full spectrum of treatment options available for runner’s knee — from the immediate self-management tools (load modification, taping, footwear adjustment) through the rehabilitation exercises (hip strengthening, VMO training, gait retraining) to the long-term prevention program (strength maintenance, load monitoring, early warning recognition) — empowers the athlete to manage this common condition with the evidence-based confidence that passive waiting for the pain to resolve cannot provide. The passive approach to runner’s knee — reducing running and hoping the pain goes away — produces temporary relief that recurs with training resumption because the underlying biomechanical causes remain unaddressed. The active rehabilitation approach — addressing hip weakness, VMO timing, gait mechanics, and load management simultaneously — produces the lasting resolution that allows return to full training without the recurrence that passive management allows. Every week of consistent rehabilitation exercise brings the runner closer to the pain-free running that is the realistic, evidence-supported outcome for the vast majority of PFPS cases. The literature on PFPS outcomes is among the most positive in sports medicine for any overuse injury — 80–90% of runners who complete appropriate conservative rehabilitation return to their pre-injury activity level within 6 months. This exceptional success rate reflects both the treatable nature of the underlying biomechanical causes and the effectiveness of the exercise-based rehabilitation approach when consistently applied. You are in the 80–90%, not the 10–20% — begin the rehabilitation program described in this article, trust the process, and claim the pain-free running that your effort will produce. The patella will thank you. The miles ahead will prove it. The training environment and running surface also deserve consideration in the prevention and rehabilitation of patellofemoral pain syndrome. Softer running surfaces — grass, dirt trails, and rubber tracks — reduce the impact forces transmitted through the lower limb compared to asphalt and concrete, potentially reducing the cumulative patellofemoral loading of the same weekly mileage on harder surfaces. Transitioning a portion of weekly running from road to trail or grass during the return-to-running phase reduces joint stress while the patellofemoral joint is still recovering — the surface change providing a form of load modification that most runners can implement without special equipment or facility access. The incline management principle applies on both road and trail: minimize descent grades during the rehabilitation phase (downhill running doubles or triples the patellofemoral joint reaction force compared to flat running at the same speed) and progressively reintroduce hills over the final weeks of the return-to-running protocol, beginning with gentle grades of 3–5% and advancing to steeper hills only after full flat-running capacity is established. The combination of these surface and gradient management principles with the exercise rehabilitation and gait retraining described in this article constitutes the complete environmental and training-structure approach to patellofemoral pain syndrome that maximizes recovery speed and minimizes recurrence risk across the return-to-running transition that marks the successful conclusion of the PFPS rehabilitation journey.

3. Treatment and Immediate Pain Relief for Runner’s Knee
The immediate management of runner’s knee aims to reduce the patellofemoral joint stress that is producing pain — creating the window of pain reduction that allows rehabilitation exercises to be performed effectively and normal function to be maintained while the underlying biomechanical causes are addressed. The treatment approaches in this section range from the immediate load modification decisions through the taping, footwear, and anti-inflammatory interventions that acute pain management employs.
Load Modification: The First and Most Important Treatment Step
The most immediately effective treatment for runner’s knee is reducing the patellofemoral joint loading that is provoking the pain — specifically, modifying the training activities that most load the patellofemoral joint while maintaining the fitness and cardiovascular conditioning that complete rest would sacrifice. The load modification hierarchy for runners with PFPS: eliminate downhill running immediately (the highest patellofemoral loading running condition — removing it alone often produces significant pain reduction within days); reduce overall running volume by 50% and avoid the pace and duration that previously provoked pain; replace running volume with swimming or pool running (eliminates the impact loading of ground running while maintaining cardiovascular fitness); and transition upper body and core strength training to maintain overall conditioning during the running load reduction phase. The stair descent modification: taking stairs one at a time with the unaffected leg leading (step-to pattern) dramatically reduces the single-leg eccentric quadricep loading that stair descent places on the patellofemoral joint — a simple daily modification that prevents the cumulative pain provocation that repeated stair use in an office building or multi-story home produces. Sitting modification: avoid sustained deep knee flexion by standing or walking every 20–30 minutes during extended sitting periods — the theatre sign physiology (pain increasing with sustained flexed-knee sitting) suggests that this positional loading contributes to cumulative patellofemoral stress, and periodic position changes reduce this contribution. From PubMed PFPS treatment research, load modification combined with targeted exercise produces superior outcomes to either approach alone — the load reduction creates the pain-free window that exercise rehabilitation requires, while the exercises address the muscular weaknesses that the load modification alone cannot resolve.
Patellar Taping and Bracing
Patellar taping — using rigid sports tape to manually reposition the patella medially (toward the center of the knee) — is one of the most effective immediate pain relief tools for PFPS, producing pain reduction that allows pain-free exercise during the period when strengthening exercises would otherwise provoke symptoms. The McConnell taping technique: with the knee in slight flexion, a strip of rigid tape is applied from the lateral border of the patella and pulled medially, repositioning the patella in the femoral groove and reducing the lateral facet loading that is producing pain. Correctly applied McConnell taping can reduce PFPS pain by 50–70% during provocative activities — allowing the runner to complete rehabilitation exercises and modified training with significantly less pain than untaped. Learning the technique: McConnell taping is most effectively taught by a physiotherapist and then self-applied once the technique is learned — the specific direction and tension of the tape application determines its effectiveness, and incorrect application does not produce the patellar repositioning benefit. Kinesiology tape (KT tape) applied in a patellar support pattern provides a gentler, more comfortable alternative that some athletes find sufficiently effective for their pain level — appropriate for mild to moderate PFPS where the precise repositioning of rigid McConnell tape is not required. Patellar tracking braces with a lateral buttress (a firm pad on the outer side of the knee that prevents lateral patellar displacement during knee flexion) provide the same mechanical repositioning benefit as taping in a pre-made support that does not require skin preparation or taping skill. For athletes who will be taping daily for weeks during rehabilitation, the skin irritation that rigid tape produces makes alternating between taping and bracing days a practical approach that maintains the mechanical benefit while allowing skin recovery.
Footwear, Orthotics, and Biomechanical Interventions
Footwear modifications and foot orthoses address the foot-to-knee kinetic chain contributions to patellofemoral pain — specifically, the excessive pronation that produces tibial internal rotation and dynamic knee valgus during running. Footwear assessment: examine the wear pattern of current running shoes (excessive medial midsole compression and heel wear indicates overpronation); check the heel counter stiffness (a collapsed heel counter fails to control subtalar motion); and consider whether the current footwear was recently changed (new footwear with different support characteristics is a common PFPS trigger). Anti-pronation footwear (motion control or stability shoes) can reduce dynamic knee valgus during running by limiting foot eversion, potentially reducing patellofemoral stress — though the evidence for footwear change as a standalone treatment for PFPS is modest, and changes should be implemented gradually (alternating new and old shoes for 2 weeks before complete transition) to avoid the adjustment-period injury that sudden footwear changes can produce. Custom orthotics — prescribed by a podiatrist after gait analysis — provide foot support specifically tailored to the individual’s biomechanical needs, and research on orthoses for PFPS finds short-term pain reduction comparable to that of exercise rehabilitation. The combination of orthotics with exercise rehabilitation produces superior outcomes to either approach alone — the orthoses address the foot mechanics contribution while the rehabilitation exercises address the hip and quadricep weakness that orthotics alone cannot correct.
The runner’s knee experience — as frustrating and limiting as it is during the acute phase — is one of the most instructive athletic experiences available precisely because it reveals the biomechanical vulnerabilities that high running volume exposes. The hip weakness, the VMO timing deficit, the gait mechanics errors, and the training load management failures that PFPS diagnoses are all correctable through the rehabilitation program described in this article — and correcting them produces a runner who is not just pain-free but fundamentally more capable, durable, and resilient than before the injury revealed these deficits. The 6–12 weeks of PFPS rehabilitation is an investment that pays compounding dividends across every subsequent year of running — the runner who does the work returns to training biomechanically stronger, technically better, and more aware of the early warning signals that allow early intervention before full PFPS recurrence. This is the silver lining of runner’s knee that most athletes discover only in retrospect: the injury that felt like a setback was actually the catalyst for the biomechanical development that prevented more serious injury and enabled the sustained high-mileage running that the pre-injury weakness would eventually have made impossible. The emotional dimension of runner’s knee cannot be overstated for athletes who define themselves through their running practice. The identity disruption, the loss of the daily ritual that running provides, the social disconnection from running partners, and the anxiety about whether full recovery is genuinely achievable — all require deliberate management alongside the physical rehabilitation. The runners who navigate PFPS most successfully share a common psychological approach: they grieve the temporary loss of running honestly rather than suppressing the frustration; they redirect their competitive instincts toward the rehabilitation program (setting PR times for the rehabilitation exercises, progressively loading the hip strength program); they maintain connection with the running community through spectating, volunteering at races, and supporting training partners even while unable to train themselves; and they use the forced reduction in running volume to invest in the cross-training, strength work, and recovery practices that busy training schedules chronically deprioritize. These psychological strategies convert the PFPS experience from a pure loss into a complex gain — the strength development, cross-training fitness, and recovery habit establishment that occur during rehabilitation produce a more complete, resilient athlete on the other side of the injury than existed before it. The rehabilitation period is the opportunity to build the foundations that sustain the running practice long-term — seize it with the same intentionality that the training that preceded the injury deserves. The evidence base for runner’s knee rehabilitation continues to grow, with emerging research on blood flow restriction training (BFR), dry needling, and shockwave therapy adding to the established exercise and biomechanical interventions. BFR training — using a blood pressure cuff or specialized tourniquet to partially restrict venous return during low-load resistance exercises — allows hip and quadricep strengthening at loads that do not provoke patellofemoral pain, producing strength gains comparable to high-load training without the joint loading that high-load exercises require. This makes BFR training particularly valuable for athletes with moderate-to-severe PFPS who cannot tolerate the knee flexion angles that standard resistance training requires during the acute rehabilitation phase. Shockwave therapy — acoustic pressure wave treatment applied to the lateral retinaculum and patellar tendon — has emerging evidence for PFPS symptom reduction in cases that do not respond to exercise rehabilitation alone. These emerging modalities supplement rather than replace the evidence-based exercise rehabilitation program described in this article — they are adjuncts for cases that require additional intervention, not alternatives to the fundamental hip strengthening and gait retraining that address the root causes of patellofemoral pain syndrome in most runners.

4. Rehabilitation Exercises: Fixing the Root Cause
The exercise rehabilitation program for runner’s knee addresses the three primary muscular contributors to patellofemoral pain: hip abductor and external rotator weakness, VMO (vastus medialis oblique) weakness and timing deficit, and overall lower limb loading mechanics. Research consistently identifies targeted exercise rehabilitation as the most effective treatment for PFPS — superior to passive modalities (ultrasound, electrical stimulation, massage) and producing outcomes comparable to surgical intervention in appropriately selected cases.
Hip Strengthening: The Foundation of Runner’s Knee Rehabilitation
Hip abductor and external rotator strengthening is the most evidence-supported single intervention for patellofemoral pain syndrome — the research on hip strengthening for PFPS consistently finds significant pain reduction and functional improvement, with effect sizes exceeding those of isolated quadricep strengthening in several randomized controlled trials. The mechanism: strengthening the gluteus medius, minimus, and hip external rotators reduces the femoral adduction and internal rotation during running that produces dynamic knee valgus and patellofemoral stress — addressing the root cause rather than the symptom. The essential hip strengthening exercises for PFPS rehabilitation: clamshells (lying on the side with hips flexed to 45 degrees, knees bent at 90 degrees, rotating the top knee upward like a clamshell opening — 3 sets of 20 repetitions per side, adding resistance band above the knees when bodyweight becomes easy); side-lying hip abduction (lying on the side with the top leg straight, lifting it 30–45 degrees off the bottom leg and slowly lowering — 3 sets of 15 per side); single-leg glute bridge (lying on the back with one knee bent foot on the floor, the other leg extended, pressing through the planted foot to lift the hips — 3 sets of 12–15 per side, progressing to elevated foot position when comfortable); and hip hike (standing on a step with one foot, dropping the non-weight-bearing hip below the step level then hiking it above level using the standing leg’s hip abductor — 3 sets of 15 per side). From ACSM exercise guidelines for PFPS, hip strengthening exercises should be performed 3 times per week, progressed over 6–8 weeks, and maintained as a permanent training program component after return to running to prevent recurrence.
Quadricep Rehabilitation: VMO Emphasis and Terminal Extension
Quadricep strengthening for PFPS focuses on both overall quadricep development and the specific activation timing of the VMO that medial patellar stabilization requires. The terminal knee extension (TKE): standing with a resistance band anchored behind the knee, stepping back to create tension, and fully extending the knee against the band resistance — emphasizing the last 30 degrees of extension where VMO activation is greatest. This exercise specifically trains the VMO in its most functionally relevant range without loading the patellofemoral joint at the high flexion angles that provoke pain. Short-arc quads: lying on the back with a rolled towel under the knee (maintaining 30–40 degrees of flexion), extending the lower leg from this position to full extension and slowly lowering — 3 sets of 15–20 repetitions. This limited-range exercise maximizes VMO activation while avoiding the deep flexion angles that produce patellofemoral pain. Step-up with VMO emphasis: stepping up onto a low step (10–15cm) with the affected leg, focusing on keeping the knee tracking over the second toe (preventing knee valgus) and consciously activating the inner thigh muscle during the step — 3 sets of 12–15 per side. The knee pain threshold during quadricep exercises should be maintained below 3/10 — exercises producing pain above this level should be modified by reducing resistance, reducing range of motion to the pain-free arc, or substituting with a less provocative variation. Gradually loading the patellofemoral joint through progressively deeper knee flexion angles (as pain tolerance allows over weeks of rehabilitation) is the progressive loading approach that restores normal joint loading capacity over the rehabilitation timeline.
Running Gait Retraining: Biomechanical Correction
Gait retraining — modifying specific running mechanics to reduce patellofemoral stress — has emerging evidence as one of the most effective interventions for PFPS, with several high-quality studies demonstrating that targeted gait cues produce significant and sustained pain reduction in runners who implement them. The most evidence-supported gait modifications for PFPS: increased step rate (increasing cadence by 5–10% from the self-selected rate — typically adding 8–10 steps per minute — reduces stride length, which reduces impact forces and the knee flexion angle at foot strike that patellofemoral loading is highest at); forward trunk lean (a slight forward lean of the trunk during running shifts load from the knee to the hip and reduces the knee flexion moment that loads the patellofemoral joint); and reduced contralateral pelvic drop (cueing the runner to keep the pelvis level rather than allowing the non-stance side to drop reduces the ipsilateral femoral adduction that dynamic knee valgus produces). The practical implementation: use a metronome app set to the target cadence (typically 170–180 steps per minute for most recreational runners) for 10-minute segments of training runs, gradually extending the metronomeed portion as the new cadence becomes automatic. Running on a treadmill with video analysis (or filming yourself from behind with a phone) allows observation of pelvic drop and knee valgus that self-perception without video cannot detect. Gait retraining requires 4–8 weeks of consistent practice before the new mechanics become automatic enough to maintain at all running speeds and conditions — short-term conscious application that builds toward unconscious competence.
Progressive Return-to-Running Protocol
The return-to-running program after PFPS rehabilitation follows a graduated exposure protocol that progressively increases patellofemoral loading while monitoring pain response. The criteria for beginning the return-to-running protocol: pain-free walking for 30 minutes; pain below 2/10 during the step-down test; hip abductor and quadricep strength at 80%+ of the unaffected side; and pain-free performance of the rehabilitation exercises at the current progression level. The 8-week return-to-running program: Week 1 — 1 minute run/2 minutes walk × 10 repetitions, every other day; Week 2 — 2 minutes run/2 minutes walk × 8; Week 3 — 3 minutes run/2 minutes walk × 6; Week 4 — 5 minutes run/2 minutes walk × 4; Week 5 — 8 minutes run/2 minutes walk × 3; Week 6 — 15 minutes continuous run; Week 7 — 20 minutes continuous run; Week 8 — 25–30 minutes continuous run. Progress to the next stage only when the current stage produces pain below 2/10 during the run and no increased pain in the 24 hours following. If any stage produces pain above 3/10 or increased next-day pain, return to the previous stage for an additional week before attempting progression. The return-to-running protocol should be performed on flat surfaces — avoid hills, particularly descents, until 4 weeks of pain-free flat running is established.
The relationship between running mechanics and patellofemoral health is bidirectional — poor mechanics produce patellofemoral overload, and patellofemoral pain alters mechanics further through pain-avoidance compensations that redistribute load to other vulnerable tissues. Breaking this cycle requires the simultaneous load reduction, strength rehabilitation, and gait retraining that the comprehensive PFPS program addresses — no single intervention alone is sufficient. The runner who understands this system — patellofemoral mechanics, the muscle contributors to those mechanics, the gait modification cues that reduce joint stress, and the training load principles that allow gradual reloading of healing tissue — has the complete knowledge framework that evidence-based PFPS management requires. Apply this framework with patience, consistency, and willingness to accept the temporary step-back in training that full rehabilitation requires, and the return to unrestricted, pain-free running that most PFPS sufferers achieve within 3–6 months of appropriate management awaits on the other side of the rehabilitation program. The biomechanical corrections from runner’s knee rehabilitation — stronger hips, better VMO timing, improved gait mechanics, more sophisticated load management — represent the running-specific athletic development that high mileage training alone cannot produce. Many runners discover that their post-rehabilitation running feels easier, more efficient, and more sustainable than pre-injury running precisely because the biomechanical efficiency that rehabilitation instills reduces the energy cost and joint stress of every stride. The running economy improvement from better mechanics and stronger hip stabilizers produces the effortless running sensation that experienced runners describe — the feeling of running with the whole body rather than just the legs, with the hips driving the movement and the knees tracking efficiently over the foot. This running efficiency is not just a performance benefit — it is the mechanical protection against patellofemoral reloading that makes the post-rehabilitation runner more durable than their pre-injury self. The investment in rehabilitation is simultaneously the investment in running efficiency — and the return on this investment compounds across every mile of the training and racing that follows. The runner who implements this complete evidence-based approach to patellofemoral pain management — combining accurate diagnosis, targeted rehabilitation, biomechanical correction, and systematic load management — achieves the lasting resolution and return to full running that the condition, properly addressed, reliably allows. Begin today. Run pain-free tomorrow.

5. Prevention and Return to Running: Long-Term Strategy and FAQs
Runner’s knee has a high recurrence rate without addressing the underlying biomechanical factors — up to 70% of PFPS cases recur within 5 years in runners who return to pre-injury training without implementing preventive strategies. The long-term prevention framework addresses training load management, permanent strength maintenance, biomechanical monitoring, and the lifestyle factors that tissue resilience depends on.
Long-Term Prevention: The Complete Strategy
Preventing runner’s knee recurrence requires maintaining the hip and quadricep strength that rehabilitation develops — the strength program that resolved the acute episode must transition from a rehabilitation intervention into a permanent training program component. The maintenance hip strength program: 2 sessions per week of the core rehabilitation exercises (clamshells, side-lying hip abduction, single-leg glute bridge, hip hike) at the maintenance dose (2 sets × 15 repetitions) provides the ongoing stimulus that prevents the strength regression to the pre-injury weakness that produced the original episode. Training load management: the 10% weekly volume increase rule — never increasing weekly running mileage by more than 10% from the previous week — prevents the overload peaks that exceed patellofemoral joint adaptation capacity. Plan deload weeks (25–50% volume reduction) every 4–6 weeks to allow accumulated patellofemoral stress to resolve before the next loading phase. The long run progression: the longest run of the week should not exceed 30% of total weekly mileage — excessively long single runs relative to total training volume produce disproportionate patellofemoral loading without the base fitness that supports it. Shoe replacement timing: running shoes lose 40–50% of their cushioning and support by 500–800km — replacing training footwear before this mileage prevents the biomechanical changes from shoe degradation that commonly trigger PFPS recurrence. Strength training integration: runners who include 2 sessions per week of lower body resistance training (squats, Romanian deadlifts, hip thrusts, single-leg exercises) demonstrate significantly lower running injury rates than those who run only — the strength training develops the muscular protection and bone density that running loads require. From American Medical Society for Sports Medicine guidelines, the most effective runner’s knee prevention program combines load management, strength training, and gait monitoring — addressing all three primary risk factor categories rather than any single contributor.
Monitoring Warning Signs: Early Intervention
The early warning signs of developing patellofemoral stress — before pain becomes the dominant symptom — allow intervention before the full PFPS syndrome is established. The early warning signals: mild anterior knee ache during or after runs that was not present previously; increased stiffness around the kneecap on waking that resolves within 10 minutes; mild theatre sign positive (slight discomfort during prolonged sitting) without significant provocation during running; and reduced tolerance for stair descent that the runner notices but does not yet classify as a significant problem. At the appearance of these early warning signals: reduce running volume by 20–30% immediately; add the hip strengthening exercises to the training program; review recent training load changes that may have introduced the patellofemoral overload; and monitor pain response over 1–2 weeks. Early intervention at the warning sign stage typically resolves the developing stress within 1–2 weeks — preventing the progression to the full symptomatic PFPS that requires 6–12 weeks of formal rehabilitation. This early-warning monitoring mindset — paying attention to the subtle signals that precede injury rather than ignoring them until they become impossible to ignore — is the most effective injury prevention approach available to any runner, for patellofemoral pain and all other running-related injuries.
Frequently Asked Questions About Runner’s Knee
Can I run through runner’s knee pain? Running through PFPS pain at 4+/10 consistently delays recovery and risks converting acute patellofemoral irritation into chronic cartilage damage. Pain below 2/10 that does not increase during or after the run is generally acceptable to train through during the early stages of rehabilitation — but any pain above this threshold requires load reduction. How long does runner’s knee take to heal? Mild PFPS (symptoms for less than 4 weeks) typically resolves with 4–6 weeks of appropriate rehabilitation. Moderate PFPS (symptoms for 4–12 weeks) requires 8–12 weeks of rehabilitation. Chronic PFPS (symptoms for more than 3 months) may require 3–6 months of consistent rehabilitation before full running capacity is restored — patience and consistency in the rehabilitation program produce the best outcomes. Is runner’s knee the same as arthritis? PFPS is not osteoarthritis — it is a pain syndrome arising from abnormal mechanical loading of a structurally normal joint. However, untreated or repeatedly recurrent PFPS is associated with increased risk of developing patellofemoral osteoarthritis in later life — another reason to address the biomechanical causes rather than managing pain and continuing to load the joint inappropriately. Should I take anti-inflammatories for runner’s knee? NSAIDs provide short-term pain relief that can allow rehabilitation exercises to be performed more comfortably — but they do not address the underlying cause and should not be used as a substitute for load modification and exercise rehabilitation. Use NSAIDs sparingly for pain management during flare-ups, not as a routine daily medication for managing running-related PFPS. Can I cycle or swim while recovering from runner’s knee? Swimming is almost universally compatible with PFPS rehabilitation — the non-weight-bearing, low patellofemoral loading nature of swimming allows cardiovascular fitness maintenance without aggravating symptoms. Cycling compatibility depends on individual pain response — some runners find cycling pain-free at moderate resistance and high cadence; others find that knee flexion at the bottom of the pedal stroke provokes patellofemoral symptoms. Start with the saddle height set high (minimizing knee flexion), low resistance, and high cadence, and assess pain response before committing to cycling as a cross-training modality. Do I need surgery for runner’s knee? The vast majority of PFPS cases resolve with conservative management — surgery is rarely indicated and produces outcomes generally no better than comprehensive exercise rehabilitation in research comparisons. Surgical intervention is considered only for cases that fail 12+ months of comprehensive conservative management, and even then the evidence for surgical superiority over continued conservative care is limited.
The community of runners who have successfully rehabilitated from runner’s knee is enormous — PFPS is so common that virtually every running club includes multiple members who have gone through this experience and returned to full training. Connecting with these athletes — through running communities, physiotherapy group sessions, or online forums — provides the social support, practical advice, and motivational reinforcement that makes the rehabilitation period more manageable and the return to running more confident. The shared experience of PFPS rehabilitation is one of the most common bonds in recreational running communities — use it as a resource, share your own experience when you emerge on the other side, and contribute to the collective running intelligence that helps the next runner with anterior knee pain navigate their recovery more effectively than they might otherwise. The long-term perspective on runner’s knee: most runners who complete appropriate rehabilitation return to their pre-injury training volumes and paces within 3–6 months, and many go on to achieve personal bests in the year following rehabilitation — the strength and biomechanical improvements producing performance gains that the pre-injury training without these foundations could not have generated. The race personal best that many runners achieve in the 12 months following PFPS rehabilitation is not coincidence — it is the measurable performance return on the hip strength, quadricep development, and gait mechanics improvement that the rehabilitation program invested in. Runner’s knee, managed correctly, is not the end of the athletic story — it is the chapter that builds the foundation for the best running of the athlete’s career. The decision to address runner’s knee comprehensively — rather than simply reducing running and waiting for pain to subside — is the most important decision a runner with PFPS makes. Comprehensive management produces lasting resolution; symptomatic management produces temporary relief followed by recurrence. The effort required for comprehensive rehabilitation is front-loaded — the first 4–6 weeks of daily hip strengthening, load modification, and gait retraining feel like significant additional work on top of the already-reduced training program. But this front-loaded effort produces the lasting change in hip strength, VMO activation, and running mechanics that prevents the recurrence cycle that symptomatic management perpetuates. The runner who invests 4–6 weeks of rehabilitation diligence saves themselves from the years of recurrent PFPS episodes that inadequate rehabilitation allows. Make the investment. Do the work. Follow the protocol. The running life on the other side of comprehensive PFPS rehabilitation — strong, efficient, pain-free, and more durable than before — is worth every clamshell, every terminal knee extension, every metronomeed run at the unfamiliar cadence that feels awkward but is building the mechanics that will carry you through thousands of future pain-free miles. Runner’s knee is treatable. You are capable of the rehabilitation it requires. The running you love is waiting for you at the end of this process — begin it today. Every step forward in rehabilitation is a step toward the running life you deserve. Keep going. Pain-free running is your goal and your right as an athlete. Claim it now. Run well, always.





