What Is a Caloric Deficit and How Do You Use It?
⚠️ Disclaimer: The information in this article is for general educational purposes only and does not constitute medical, nutritional, or professional fitness advice. Individual results may vary. Always consult a qualified healthcare professional or certified fitness trainer before starting any new exercise program, changing your diet, or making decisions about injury treatment or recovery. If you experience pain, discomfort, or any unusual symptoms during exercise, stop immediately and seek professional guidance.

What Is a Caloric Deficit and Why It Causes Fat Loss
A caloric deficit exists when the total energy consumed through food and drink is less than the total energy the body expends through metabolism and physical activity. This energy imbalance — consuming less energy than is used — forces the body to draw on stored energy reserves to meet its ongoing metabolic demands. The primary stored energy reserves are adipose tissue (body fat) and, to a lesser extent, glycogen in the liver and muscles. When the deficit is maintained over time and protein intake is adequate, the body preferentially mobilizes fat for energy, producing the fat loss that is the primary goal of caloric deficit eating.
The physics of fat loss are well-established: one kilogram of adipose tissue contains approximately 7,700 calories of stored energy. A daily deficit of 500 calories therefore produces approximately one kilogram of fat loss every 15 days, or approximately 2 kilograms per month — the commonly cited 0.5 to 1 percent of bodyweight per week that research identifies as the optimal fat loss rate for minimizing muscle loss. This calculation is an approximation — actual fat loss rates vary with metabolic adaptation, water weight fluctuations, and the composition of the energy deficit — but provides the framework for setting deficit targets and evaluating whether the actual rate of fat loss is consistent with the intended deficit magnitude.
The Thermodynamic Basis
The first law of thermodynamics — energy is neither created nor destroyed, only converted between forms — provides the unassailable physical basis for the caloric deficit principle. The human body cannot metabolize fat without a caloric deficit, regardless of which macronutrients are consumed, what hormonal state is present, or what specific foods are eaten. Dietary strategies that claim to produce fat loss without a caloric deficit are misattributing the fat loss they observe to specific mechanisms (ketosis, intermittent fasting, hormonal changes) that in reality produce fat loss only through the caloric deficit they create. The mechanism varies; the requirement for a caloric deficit does not. This does not make all dietary approaches equivalent — the adherence, muscle preservation, and health outcomes of different deficit-creating approaches vary substantially — but it establishes that the caloric deficit is the fundamental variable that all fat loss interventions must address.
How the Body Responds to a Caloric Deficit
The body’s response to sustained caloric deficit is not passive fat mobilization — it involves active regulatory adjustments that affect both the magnitude of fat loss and the composition of weight lost. Within 2 to 4 weeks of beginning a caloric deficit, metabolic adaptation begins: resting metabolic rate decreases by 5 to 15 percent as the body reduces energy expenditure in response to reduced energy availability. Non-exercise activity thermogenesis (NEAT) — the energy burned through unconscious daily movement — decreases by 100 to 400 calories per day as reduced energy availability produces reduced spontaneous activity. Hunger hormones (ghrelin) increase and satiety hormones (leptin) decrease, amplifying appetite and reducing satiety to defend body weight. These adaptations are not indicators that the deficit has failed; they are expected physiological responses that require monitoring and periodic dietary adjustment to maintain effective fat loss over extended deficit periods.
The Role of Macronutrients in a Caloric Deficit
While total caloric intake is the primary determinant of fat loss, macronutrient composition within the deficit significantly affects muscle preservation, satiety, and adherence. Protein intake is the most critical macronutrient in a deficit: consuming 1.8 to 2.4 grams of protein per kilogram of bodyweight daily maximally stimulates muscle protein synthesis, providing the anabolic signal needed to preserve muscle tissue despite the catabolic environment of caloric restriction. Research published in the American Journal of Clinical Nutrition found that high-protein diets during caloric restriction produce significantly greater lean mass preservation than moderate-protein diets at equivalent caloric deficits — the most important single dietary modification for ensuring that weight lost comes predominantly from fat rather than muscle.
Caloric Deficit vs. Fasting
Intermittent fasting produces fat loss through the caloric deficit it creates — by restricting the hours during which eating is permitted, total daily caloric intake typically decreases spontaneously. Research comparing intermittent fasting to continuous caloric restriction at equivalent deficits finds similar fat loss outcomes and similar muscle preservation outcomes, with the primary difference being adherence: some people find time-restricted eating easier to maintain than continuous caloric monitoring, while others find continuous moderate restriction more comfortable than periods of complete fasting. The method that creates the caloric deficit most sustainably for the individual is the most effective method — not because fasting or restriction has any metabolic advantage over the other, but because the sustainable approach produces more total deficit over time.
Deep Dive: The Science of Metabolic Adaptation
Metabolic adaptation — the body’s downregulation of energy expenditure in response to caloric restriction — is the primary reason that extended caloric deficits produce progressively slower fat loss over time. Understanding the specific components of metabolic adaptation allows targeted strategies to minimize its impact and maintain fat loss rate through longer deficit phases.
The four components of metabolic adaptation: (1) Reduced resting metabolic rate from decreased lean mass — the body preferentially catabolizes muscle during a caloric deficit, and each kilogram of muscle lost reduces BMR by approximately 13 calories per day. This is the component most controllable through adequate protein and resistance training. (2) Adaptive thermogenesis — the body reduces thermogenic activity (heat production, fidgeting, organ function) by 100 to 400 calories per day in response to extended restriction. This component is largely involuntary and persists for months after deficit cessation. (3) Reduced NEAT — lower energy availability reduces spontaneous daily movement by 100 to 400 calories without conscious awareness. Taking deliberate steps to maintain NEAT through regular walking partially offsets this component. (4) Reduced exercise energy expenditure — as body weight decreases, the caloric cost of exercise decreases proportionally (moving a lighter body requires less energy). Recalculating TDEE based on reduced body weight and adjusting caloric targets accordingly is the straightforward response to this component.
The cumulative effect of these four components can reduce TDEE by 300 to 600 calories below what TDEE calculation formulas predict after 8 to 12 weeks of restriction — explaining why fat loss slows despite apparent adherence to the original deficit. Accounting for this adaptation through progressive deficit recalibration, planned diet breaks, and consistency in resistance training and protein intake produces better long-term fat loss outcomes than fighting an unchanged deficit against a significantly reduced TDEE.
Practical FAQ
How long should you stay in a caloric deficit?
Most research and practice suggests deficit phases of 8 to 16 weeks followed by a maintenance phase of at least 4 to 8 weeks before resuming restriction. Extended deficits beyond 16 weeks produce compounding metabolic adaptation, hormonal disruption, and psychological restriction fatigue that make additional fat loss increasingly difficult and the quality of life impact increasingly significant. Periodic maintenance phases allow metabolic recovery, hormonal normalization, and psychological restoration that makes subsequent deficit phases more effective and more tolerable.
Why am I not losing weight in a caloric deficit?
The most common reasons: inaccurate calorie tracking (the most frequent cause, resolvable by using a food scale for 2 weeks), metabolic adaptation that has reduced TDEE below the target caloric intake, water retention from dietary sodium or hormonal cycles masking fat loss on the scale (resolvable by tracking weekly averages over 4 weeks), or the deficit is genuinely too small to produce measurable scale changes on a weekly basis. Systematically addressing each of these possibilities — accurate tracking first, then assessing weekly trend data before making dietary adjustments — resolves the vast majority of apparent fat loss stalls.
Can you gain muscle while in a caloric deficit?
Yes, under specific conditions: beginners with significant fat stores, people returning to training after an extended break, and people with high body fat percentages can gain muscle while losing fat — a phenomenon called body recomposition. This simultaneous muscle gain and fat loss becomes progressively less achievable as training experience increases and body fat decreases toward lean levels, but it remains possible for a significant portion of recreational trainees, particularly those who combine high protein intake with consistent resistance training during their deficit phase. For leaner, more experienced trainees, the priority shifts to maximum muscle preservation during fat loss rather than muscle gain, which is the realistic outcome of an optimized deficit approach for this population.
How to Calculate Your Personal Caloric Deficit
Calculating a caloric deficit requires two values: total daily energy expenditure (TDEE — the total calories the body uses in a day) and the target caloric intake below TDEE. TDEE is estimated rather than measured for most people, with several calculation methods providing approximations that can be refined through tracking real-world weight change over time.
Calculating Basal Metabolic Rate (BMR)
Basal metabolic rate — the energy the body uses at complete rest to maintain basic physiological functions — is the foundation of TDEE calculation. The Mifflin-St Jeor equation is the most validated formula for BMR estimation in the general population:
For men: BMR = (10 × weight in kg) + (6.25 × height in cm) − (5 × age in years) + 5
For women: BMR = (10 × weight in kg) + (6.25 × height in cm) − (5 × age in years) − 161
Example: a 30-year-old man, 80kg, 180cm: BMR = (10 × 80) + (6.25 × 180) − (5 × 30) + 5 = 800 + 1,125 − 150 + 5 = 1,780 calories. This BMR represents the minimum caloric intake for basic bodily functions at complete rest — actual daily expenditure is substantially higher due to the energy cost of daily activity.
Calculating Total Daily Energy Expenditure (TDEE)
TDEE is estimated by multiplying BMR by an activity multiplier that reflects physical activity level: Sedentary (desk job, no exercise): BMR × 1.2. Lightly active (exercise 1 to 3 days/week): BMR × 1.375. Moderately active (exercise 3 to 5 days/week): BMR × 1.55. Very active (hard exercise 6 to 7 days/week): BMR × 1.725. Extremely active (physical job + daily training): BMR × 1.9.
Using the example above: 1,780 × 1.55 (moderately active) = 2,759 calories. This person’s TDEE is approximately 2,759 calories — they should consume this amount to maintain their current weight. A 500-calorie daily deficit produces a caloric intake of 2,259 calories, targeting approximately 0.5kg of fat loss per week.
Validating the Calculation Through Real-World Tracking
TDEE calculations are estimates with accuracy varying by 10 to 20 percent between individuals due to differences in metabolic efficiency, muscle mass, non-exercise activity, and hormonal factors. The most accurate approach is to use the TDEE calculation as a starting estimate and validate it through 2 to 3 weeks of consistent calorie tracking at the estimated maintenance level (without attempting a deficit): if body weight remains stable, the TDEE estimate is accurate; if weight consistently increases, TDEE is lower than estimated; if weight consistently decreases, TDEE is higher than estimated. Adjusting the TDEE estimate based on this real-world data produces a personalized caloric target that is significantly more accurate than any formula can achieve for individuals who vary substantially from the “average person” the formula was developed on.
Calorie Tracking Tools and Methods
Accurate calorie tracking requires a food scale, a nutritional database, and consistent tracking behavior. Weighing food provides substantially more accurate calorie estimates than volume measurements (cups, tablespoons) due to the density variation within food categories. Nutritional database apps (MyFitnessPal, Cronometer, MacroFactor) provide searchable databases covering most foods and branded products. Tracking consistently — including oils used in cooking, beverages, and condiments that are commonly omitted — provides more useful data than tracking some meals meticulously and estimating others. The goal of calorie tracking is not perfect accuracy but sufficient accuracy to confirm the deficit is being maintained and to identify the dietary patterns that consistently produce the intended deficit.
The Psychology of Successful Deficit Eating
The behavioral and psychological aspects of maintaining a caloric deficit are as important as the physiological aspects — and substantially underrepresented in most fat loss guidance that focuses almost exclusively on the dietary mechanics. Research from the behavioral psychology of eating identifies several patterns that reliably predict deficit adherence success: all-or-nothing thinking (treating a single off-plan meal as a failed day and abandoning the deficit for the remainder of that day or week) is associated with significantly worse outcomes than flexible restraint (acknowledging the off-plan meal and returning to the plan at the next eating opportunity without guilt or overcompensation). Planning for planned indulgences — scheduling higher-calorie meals or days in advance rather than having them occur reactively — maintains the sense of dietary control that predicts long-term adherence while accommodating the social and emotional dimensions of eating that pure dietary restriction ignores.
The identity-based approach to deficit eating — framing healthy eating as an expression of who you are rather than a set of rules you are following — produces more consistent adherence than willpower-based approaches that treat each food decision as a battle between desire and discipline. “I eat in a way that supports my health and fitness goals” is a more durable motivational frame than “I am not allowed to eat that” — the former comes from internal identity, the latter from external restriction. Building the identity of someone who eats intentionally and healthily — through consistent behavior that reinforces this identity over weeks and months — creates the automatic behavioral tendencies that maintain caloric awareness without continuous active effort.
Practical FAQ
How long should you stay in a caloric deficit?
Most research and practice suggests deficit phases of 8 to 16 weeks followed by a maintenance phase of at least 4 to 8 weeks before resuming restriction. Extended deficits beyond 16 weeks produce compounding metabolic adaptation, hormonal disruption, and psychological restriction fatigue that make additional fat loss increasingly difficult and the quality of life impact increasingly significant. Periodic maintenance phases allow metabolic recovery, hormonal normalization, and psychological restoration that makes subsequent deficit phases more effective and more tolerable.
Why am I not losing weight in a caloric deficit?
The most common reasons: inaccurate calorie tracking (the most frequent cause, resolvable by using a food scale for 2 weeks), metabolic adaptation that has reduced TDEE below the target caloric intake, water retention from dietary sodium or hormonal cycles masking fat loss on the scale (resolvable by tracking weekly averages over 4 weeks), or the deficit is genuinely too small to produce measurable scale changes on a weekly basis. Systematically addressing each of these possibilities — accurate tracking first, then assessing weekly trend data before making dietary adjustments — resolves the vast majority of apparent fat loss stalls.
Can you gain muscle while in a caloric deficit?
Yes, under specific conditions: beginners with significant fat stores, people returning to training after an extended break, and people with high body fat percentages can gain muscle while losing fat — a phenomenon called body recomposition. This simultaneous muscle gain and fat loss becomes progressively less achievable as training experience increases and body fat decreases toward lean levels, but it remains possible for a significant portion of recreational trainees, particularly those who combine high protein intake with consistent resistance training during their deficit phase. For leaner, more experienced trainees, the priority shifts to maximum muscle preservation during fat loss rather than muscle gain, which is the realistic outcome of an optimized deficit approach for this population.
How Large Should Your Deficit Be?
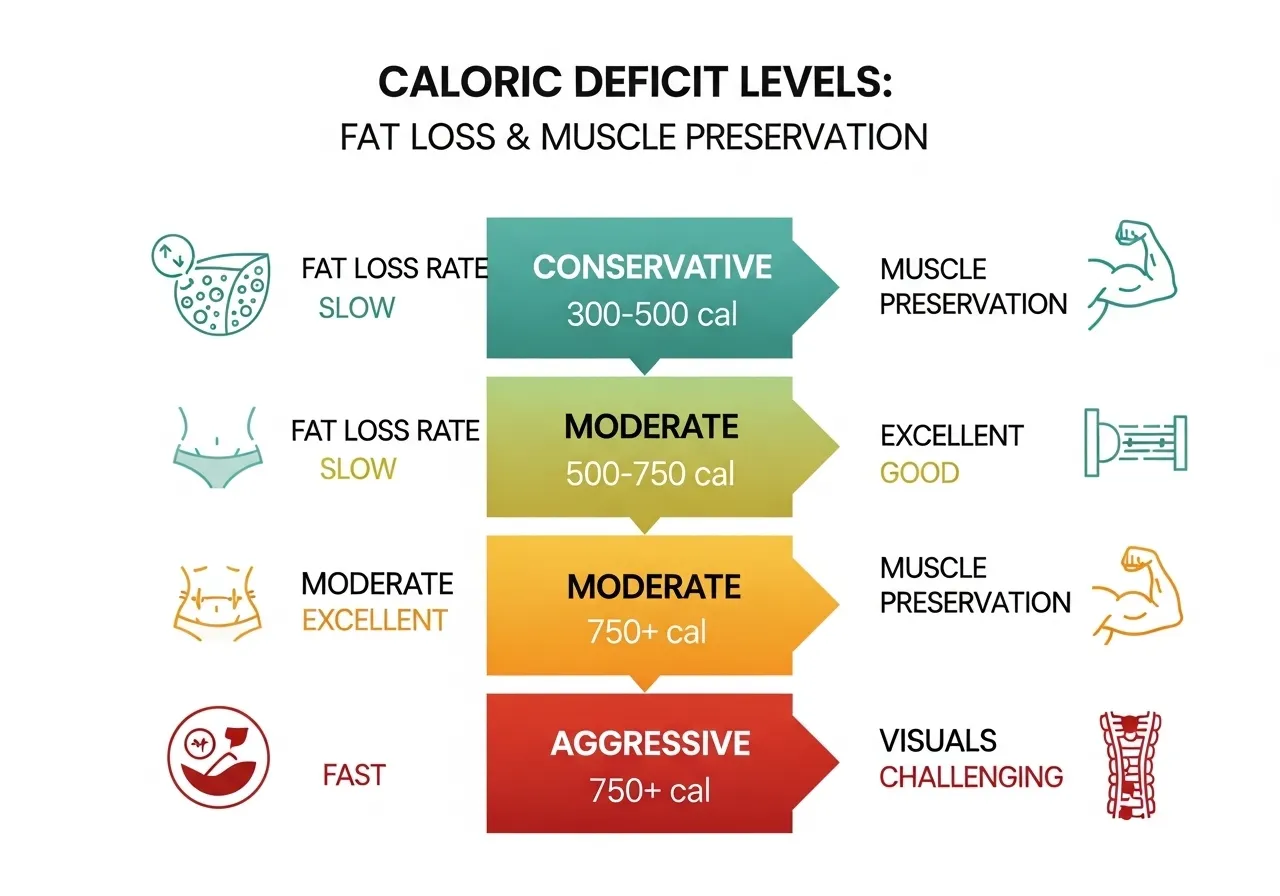
The magnitude of the caloric deficit is the single most impactful decision in fat loss planning, determining both the rate of fat loss and the degree to which muscle, performance, and wellbeing are preserved during the process. Deficit size exists on a spectrum from mild (less than 300 calories, producing slow fat loss with minimal muscle impact) to aggressive (more than 750 calories, producing faster fat loss with increased muscle loss risk and adherence difficulty).
The Conservative Deficit: 300 to 500 Calories Below TDEE
A conservative deficit of 300 to 500 calories below TDEE targets fat loss of 0.3 to 0.5 kg per week — the rate associated with the highest lean mass preservation in research, the least hunger and energy impairment, the most sustainable adherence, and the smallest metabolic adaptation response. Research published in the British Journal of Sports Medicine recommends this deficit range for most recreational trainees pursuing fat loss alongside strength training, as it produces meaningful fat loss without the performance impairment that larger deficits create. For a 75kg person, this represents a daily intake of approximately 300 to 500 calories below calculated TDEE — a reduction achievable through modest portion adjustments without dramatic dietary restriction.
The Moderate Deficit: 500 to 750 Calories Below TDEE
A moderate deficit of 500 to 750 calories below TDEE targets fat loss of 0.5 to 0.75 kg per week — the most commonly recommended deficit range for general fat loss goals. This deficit range produces meaningful, visible weekly progress while remaining achievable with most dietary patterns and typically manageable alongside regular exercise. The risk of muscle loss at this deficit range is moderate — primarily a concern when combined with inadequate protein intake or very low training frequency. High protein intake (2.0 to 2.4g/kg) significantly reduces muscle loss risk at this deficit level, making protein adequacy the most important dietary variable alongside the deficit itself.
The Aggressive Deficit: 750+ Calories Below TDEE
Deficits exceeding 750 calories below TDEE — often called “crash dieting” in casual discourse — produce faster initial fat loss but at costs that frequently undermine long-term outcomes: significant muscle loss, pronounced metabolic adaptation that slows fat loss over weeks, severe hunger that impairs adherence, reduced training performance, hormonal disruptions (reduced testosterone, elevated cortisol, impaired thyroid function), and the psychological restriction-rebound cycle that produces rapid weight regain after the aggressive restriction phase ends. Research consistently shows that aggressive deficits produce similar or worse 6-month fat loss outcomes compared to moderate deficits, despite faster initial weight loss, due to the adherence failures and metabolic adaptations they trigger. Aggressive deficits are occasionally appropriate for specific medical contexts under professional supervision; they are rarely optimal for recreational fat loss goals.
Maintenance Calories: Avoiding Under-Eating
A commonly overlooked deficit-related mistake is inadvertently creating a deficit that is too large by combining intentional dietary restriction with high training volume. Someone who targets a 500-calorie deficit through dietary adjustment and then adds 5 training sessions per week that burn 400 to 600 calories each has created a total deficit of 900 to 1,100 calories — far larger than intended and potentially exceeding the threshold that causes muscle loss and metabolic adaptation. Recalculating TDEE to include added training volume, and adjusting dietary intake upward to maintain the intended deficit magnitude, prevents this common over-restriction error.
Deep Dive: The Science of Metabolic Adaptation
Metabolic adaptation — the body’s downregulation of energy expenditure in response to caloric restriction — is the primary reason that extended caloric deficits produce progressively slower fat loss over time. Understanding the specific components of metabolic adaptation allows targeted strategies to minimize its impact and maintain fat loss rate through longer deficit phases.
The four components of metabolic adaptation: (1) Reduced resting metabolic rate from decreased lean mass — the body preferentially catabolizes muscle during a caloric deficit, and each kilogram of muscle lost reduces BMR by approximately 13 calories per day. This is the component most controllable through adequate protein and resistance training. (2) Adaptive thermogenesis — the body reduces thermogenic activity (heat production, fidgeting, organ function) by 100 to 400 calories per day in response to extended restriction. This component is largely involuntary and persists for months after deficit cessation. (3) Reduced NEAT — lower energy availability reduces spontaneous daily movement by 100 to 400 calories without conscious awareness. Taking deliberate steps to maintain NEAT through regular walking partially offsets this component. (4) Reduced exercise energy expenditure — as body weight decreases, the caloric cost of exercise decreases proportionally (moving a lighter body requires less energy). Recalculating TDEE based on reduced body weight and adjusting caloric targets accordingly is the straightforward response to this component.
The cumulative effect of these four components can reduce TDEE by 300 to 600 calories below what TDEE calculation formulas predict after 8 to 12 weeks of restriction — explaining why fat loss slows despite apparent adherence to the original deficit. Accounting for this adaptation through progressive deficit recalibration, planned diet breaks, and consistency in resistance training and protein intake produces better long-term fat loss outcomes than fighting an unchanged deficit against a significantly reduced TDEE.
Practical FAQ
How long should you stay in a caloric deficit?
Most research and practice suggests deficit phases of 8 to 16 weeks followed by a maintenance phase of at least 4 to 8 weeks before resuming restriction. Extended deficits beyond 16 weeks produce compounding metabolic adaptation, hormonal disruption, and psychological restriction fatigue that make additional fat loss increasingly difficult and the quality of life impact increasingly significant. Periodic maintenance phases allow metabolic recovery, hormonal normalization, and psychological restoration that makes subsequent deficit phases more effective and more tolerable.
Why am I not losing weight in a caloric deficit?
The most common reasons: inaccurate calorie tracking (the most frequent cause, resolvable by using a food scale for 2 weeks), metabolic adaptation that has reduced TDEE below the target caloric intake, water retention from dietary sodium or hormonal cycles masking fat loss on the scale (resolvable by tracking weekly averages over 4 weeks), or the deficit is genuinely too small to produce measurable scale changes on a weekly basis. Systematically addressing each of these possibilities — accurate tracking first, then assessing weekly trend data before making dietary adjustments — resolves the vast majority of apparent fat loss stalls.
Can you gain muscle while in a caloric deficit?
Yes, under specific conditions: beginners with significant fat stores, people returning to training after an extended break, and people with high body fat percentages can gain muscle while losing fat — a phenomenon called body recomposition. This simultaneous muscle gain and fat loss becomes progressively less achievable as training experience increases and body fat decreases toward lean levels, but it remains possible for a significant portion of recreational trainees, particularly those who combine high protein intake with consistent resistance training during their deficit phase. For leaner, more experienced trainees, the priority shifts to maximum muscle preservation during fat loss rather than muscle gain, which is the realistic outcome of an optimized deficit approach for this population.
What to Eat in a Caloric Deficit (Without Losing Muscle)
The composition of the caloric deficit determines whether the weight lost consists primarily of fat or includes significant muscle loss — the single most important qualitative distinction in fat loss that the simple caloric deficit calculation does not capture. A caloric deficit achieved through low-protein, low-training approaches produces weight loss with significant muscle loss; the same deficit achieved through high-protein, resistance-training approaches produces weight loss with minimal muscle loss. These outcomes look identical on a scale but represent dramatically different body composition changes.
The High-Protein Deficit Template
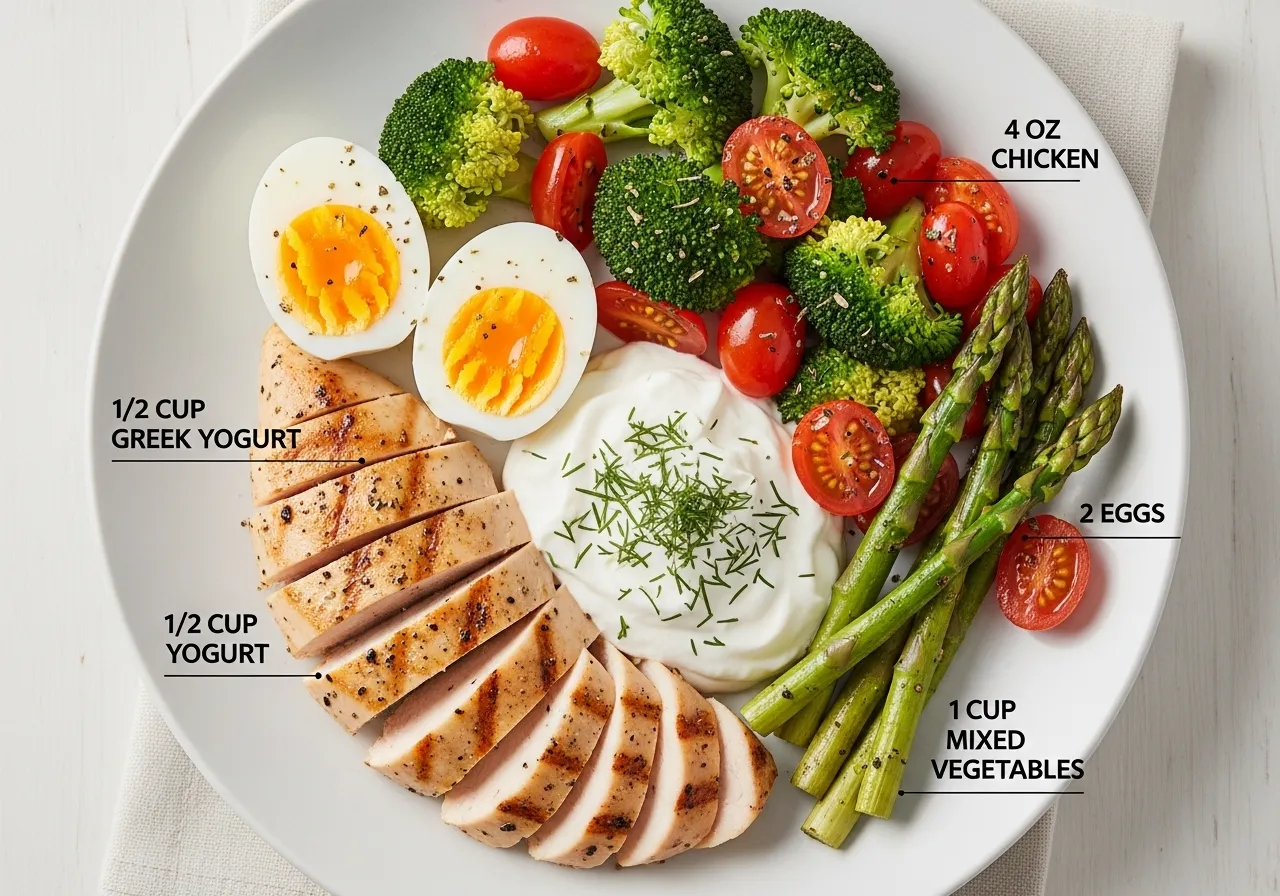
The most research-supported dietary template for fat loss with muscle preservation: protein at 2.0 to 2.4g/kg bodyweight per day (the most critical variable — higher than general health recommendations to compensate for the catabolic stress of the caloric deficit), carbohydrates at 2 to 4g/kg/day (providing the glycogen needed to maintain training performance), fat at 0.8 to 1.2g/kg/day (the minimum needed to support hormonal function and fat-soluble vitamin absorption). For an 80kg person targeting maintenance: 160 to 192g protein (640 to 768 calories), 160 to 320g carbohydrates (640 to 1,280 calories), 64 to 96g fat (576 to 864 calories) — total 1,856 to 2,912 calories, adjusted to the target deficit-appropriate intake. Protein fills the caloric floor regardless of the total target, with carbohydrates and fat adjusted to meet the remaining caloric budget.
High-Volume, Low-Calorie Foods That Reduce Hunger
Managing hunger while maintaining a caloric deficit is the central adherence challenge of fat loss, and the most effective dietary strategy is building meals around high-volume, low-calorie foods that create physical stomach fullness disproportionate to their caloric contribution. Non-starchy vegetables — cucumber, celery, lettuce, zucchini, tomatoes, mushrooms — provide 15 to 35 calories per 100g while adding significant volume and fiber that slows gastric emptying and reduces appetite. Broth-based soups provide satiety through volume and heat effects at very low caloric density. Lean white fish (tilapia, cod, pollock) provides 20 to 22g of protein per 100g at approximately 80 to 100 calories — the most protein-dense, calorie-efficient animal protein source available. Building each meal around these high-volume foods before adding calorie-dense components allows satisfying plate volumes within restricted caloric targets.
Food Timing in a Caloric Deficit
Protein distribution across the day becomes more important during a caloric deficit because muscle protein synthesis rates are reduced by caloric restriction and must be maximally stimulated by each protein-containing meal to maintain muscle mass. Consuming 30 to 40g of high-quality protein at each of 4 to 5 meals — rather than consuming the same total protein in fewer, larger servings — maximizes the number of daily muscle protein synthesis stimulations and produces superior muscle preservation at equivalent total protein intake. Front-loading carbohydrates toward training session windows (consuming the majority of daily carbohydrates around the time of training) and reducing carbohydrate intake in the hours furthest from training optimizes performance without changing total daily caloric intake.
The Psychology of Successful Deficit Eating
The behavioral and psychological aspects of maintaining a caloric deficit are as important as the physiological aspects — and substantially underrepresented in most fat loss guidance that focuses almost exclusively on the dietary mechanics. Research from the behavioral psychology of eating identifies several patterns that reliably predict deficit adherence success: all-or-nothing thinking (treating a single off-plan meal as a failed day and abandoning the deficit for the remainder of that day or week) is associated with significantly worse outcomes than flexible restraint (acknowledging the off-plan meal and returning to the plan at the next eating opportunity without guilt or overcompensation). Planning for planned indulgences — scheduling higher-calorie meals or days in advance rather than having them occur reactively — maintains the sense of dietary control that predicts long-term adherence while accommodating the social and emotional dimensions of eating that pure dietary restriction ignores.
The identity-based approach to deficit eating — framing healthy eating as an expression of who you are rather than a set of rules you are following — produces more consistent adherence than willpower-based approaches that treat each food decision as a battle between desire and discipline. “I eat in a way that supports my health and fitness goals” is a more durable motivational frame than “I am not allowed to eat that” — the former comes from internal identity, the latter from external restriction. Building the identity of someone who eats intentionally and healthily — through consistent behavior that reinforces this identity over weeks and months — creates the automatic behavioral tendencies that maintain caloric awareness without continuous active effort.
Practical FAQ
How long should you stay in a caloric deficit?
Most research and practice suggests deficit phases of 8 to 16 weeks followed by a maintenance phase of at least 4 to 8 weeks before resuming restriction. Extended deficits beyond 16 weeks produce compounding metabolic adaptation, hormonal disruption, and psychological restriction fatigue that make additional fat loss increasingly difficult and the quality of life impact increasingly significant. Periodic maintenance phases allow metabolic recovery, hormonal normalization, and psychological restoration that makes subsequent deficit phases more effective and more tolerable.
Why am I not losing weight in a caloric deficit?
The most common reasons: inaccurate calorie tracking (the most frequent cause, resolvable by using a food scale for 2 weeks), metabolic adaptation that has reduced TDEE below the target caloric intake, water retention from dietary sodium or hormonal cycles masking fat loss on the scale (resolvable by tracking weekly averages over 4 weeks), or the deficit is genuinely too small to produce measurable scale changes on a weekly basis. Systematically addressing each of these possibilities — accurate tracking first, then assessing weekly trend data before making dietary adjustments — resolves the vast majority of apparent fat loss stalls.
Can you gain muscle while in a caloric deficit?
Yes, under specific conditions: beginners with significant fat stores, people returning to training after an extended break, and people with high body fat percentages can gain muscle while losing fat — a phenomenon called body recomposition. This simultaneous muscle gain and fat loss becomes progressively less achievable as training experience increases and body fat decreases toward lean levels, but it remains possible for a significant portion of recreational trainees, particularly those who combine high protein intake with consistent resistance training during their deficit phase. For leaner, more experienced trainees, the priority shifts to maximum muscle preservation during fat loss rather than muscle gain, which is the realistic outcome of an optimized deficit approach for this population.
Common Mistakes People Make in a Caloric Deficit
The difference between successful and unsuccessful fat loss attempts is most often not motivation or effort but the specific mistakes that derail adherence, slow progress, or undermine the health outcomes that should accompany fat loss. Understanding these mistakes before beginning a caloric deficit program allows proactive prevention rather than reactive troubleshooting after progress has stalled.
Underestimating Caloric Intake
Research consistently shows that people underestimate their caloric intake by 20 to 50 percent, with the greatest underestimation occurring in the high-calorie foods most likely to sabotage a deficit: cooking oils (120 calories per tablespoon, often used in quantities of 3 to 5 tablespoons per meal), nut butters (190 calories per 2 tablespoons, often consumed in much larger amounts), alcohol (150 to 200 calories per standard drink, not included in most dietary tracking), and condiments and dressings (100 to 300 calories per serving, frequently omitted from tracking). Using a food scale and tracking everything — including cooking oils, beverages, and condiments — for at least 2 to 4 weeks provides the accurate caloric awareness that allows effective deficit management without continuous tracking thereafter.
Cutting Calories Without Increasing Protein
The most consequential mistake in caloric deficit eating is reducing total calories without proportionally increasing protein intake. When total calories decrease while protein remains at maintenance levels (1.2 to 1.6g/kg), the percentage of daily calories from protein increases on paper but the absolute protein intake may remain below the threshold needed for muscle preservation during caloric restriction. The correct approach is to increase absolute protein intake during a deficit — to 2.0 to 2.4g/kg — while reducing carbohydrates and fat to create the caloric deficit. This reallocation maintains the muscle-protective protein intake while achieving the caloric reduction needed for fat loss.
Neglecting Resistance Training
Caloric deficit without resistance training produces weight loss that includes significant muscle loss alongside fat loss — a body composition outcome that reduces resting metabolic rate (muscle burns more calories at rest than fat), reduces physical capability, and creates the “skinny fat” appearance that most fat loss pursuits are trying to avoid. Resistance training during a caloric deficit provides the muscle-preserving mechanical stimulus that, combined with adequate protein intake, maintains lean mass while fat is lost. Even 2 resistance training sessions per week produces meaningful muscle preservation benefits during fat loss compared to cardio-only or no-training deficit approaches.
Expecting Linear Progress
Body weight fluctuates by 1 to 3 kg daily due to water retention from dietary sodium, glycogen storage and depletion, digestive system contents, and hormonal water retention cycles — fluctuations that are entirely unrelated to actual fat loss or gain. Interpreting these normal fluctuations as failure, and abandoning the deficit in response to a temporary scale increase, is the most common cause of premature program abandonment. Tracking weekly average weight (the average of 7 daily weigh-ins) rather than individual daily weigh-ins eliminates the noise of daily fluctuation and reveals the genuine fat loss trend that individual measurements cannot reliably show.
Deep Dive: The Science of Metabolic Adaptation
Metabolic adaptation — the body’s downregulation of energy expenditure in response to caloric restriction — is the primary reason that extended caloric deficits produce progressively slower fat loss over time. Understanding the specific components of metabolic adaptation allows targeted strategies to minimize its impact and maintain fat loss rate through longer deficit phases.
The four components of metabolic adaptation: (1) Reduced resting metabolic rate from decreased lean mass — the body preferentially catabolizes muscle during a caloric deficit, and each kilogram of muscle lost reduces BMR by approximately 13 calories per day. This is the component most controllable through adequate protein and resistance training. (2) Adaptive thermogenesis — the body reduces thermogenic activity (heat production, fidgeting, organ function) by 100 to 400 calories per day in response to extended restriction. This component is largely involuntary and persists for months after deficit cessation. (3) Reduced NEAT — lower energy availability reduces spontaneous daily movement by 100 to 400 calories without conscious awareness. Taking deliberate steps to maintain NEAT through regular walking partially offsets this component. (4) Reduced exercise energy expenditure — as body weight decreases, the caloric cost of exercise decreases proportionally (moving a lighter body requires less energy). Recalculating TDEE based on reduced body weight and adjusting caloric targets accordingly is the straightforward response to this component.
The cumulative effect of these four components can reduce TDEE by 300 to 600 calories below what TDEE calculation formulas predict after 8 to 12 weeks of restriction — explaining why fat loss slows despite apparent adherence to the original deficit. Accounting for this adaptation through progressive deficit recalibration, planned diet breaks, and consistency in resistance training and protein intake produces better long-term fat loss outcomes than fighting an unchanged deficit against a significantly reduced TDEE.
Practical FAQ
How long should you stay in a caloric deficit?
Most research and practice suggests deficit phases of 8 to 16 weeks followed by a maintenance phase of at least 4 to 8 weeks before resuming restriction. Extended deficits beyond 16 weeks produce compounding metabolic adaptation, hormonal disruption, and psychological restriction fatigue that make additional fat loss increasingly difficult and the quality of life impact increasingly significant. Periodic maintenance phases allow metabolic recovery, hormonal normalization, and psychological restoration that makes subsequent deficit phases more effective and more tolerable.
Why am I not losing weight in a caloric deficit?
The most common reasons: inaccurate calorie tracking (the most frequent cause, resolvable by using a food scale for 2 weeks), metabolic adaptation that has reduced TDEE below the target caloric intake, water retention from dietary sodium or hormonal cycles masking fat loss on the scale (resolvable by tracking weekly averages over 4 weeks), or the deficit is genuinely too small to produce measurable scale changes on a weekly basis. Systematically addressing each of these possibilities — accurate tracking first, then assessing weekly trend data before making dietary adjustments — resolves the vast majority of apparent fat loss stalls.
Can you gain muscle while in a caloric deficit?
Yes, under specific conditions: beginners with significant fat stores, people returning to training after an extended break, and people with high body fat percentages can gain muscle while losing fat — a phenomenon called body recomposition. This simultaneous muscle gain and fat loss becomes progressively less achievable as training experience increases and body fat decreases toward lean levels, but it remains possible for a significant portion of recreational trainees, particularly those who combine high protein intake with consistent resistance training during their deficit phase. For leaner, more experienced trainees, the priority shifts to maximum muscle preservation during fat loss rather than muscle gain, which is the realistic outcome of an optimized deficit approach for this population.

Managing Hunger and Adherence in a Caloric Deficit
Hunger — the physiological drive to eat produced by the hormonal and metabolic consequences of caloric restriction — is the primary reason that caloric deficits fail. No amount of motivation, planning, or dietary knowledge overcomes a sustained hunger level that exceeds the individual’s capacity for voluntary restriction. Managing hunger proactively — through food choices, meal timing, protein distribution, and lifestyle factors — is therefore the most practically important skill in successful deficit maintenance.
The Satiety Hierarchy of Foods
Different foods produce very different satiety responses per calorie, and building meals around high-satiety, low-calorie foods is the most effective hunger management strategy available. The protein-satiety relationship is the most powerful: protein produces greater satiety per calorie than any other macronutrient, through multiple mechanisms including slower digestion, greater thermogenesis, and direct effects on satiety hormones. Fiber is the second most powerful satiety tool: viscous soluble fiber (from oats, legumes, flaxseed) forms a gel in the digestive tract that slows gastric emptying and reduces post-meal hunger for 4 to 6 hours. Volume eating — building meals with large quantities of non-starchy vegetables — provides physical fullness disproportionate to caloric contribution through gastric stretch receptors that respond to volume regardless of caloric content.
Meal Frequency and Hunger Management
Meal frequency affects hunger management primarily through its effect on blood glucose stability and the prevention of the extreme hunger that follows extended fasting periods. Eating 3 to 5 meals per day (spaced 3 to 5 hours apart) maintains more stable blood glucose than eating 1 to 2 large meals, preventing the reactive hypoglycemia and associated extreme hunger that often drives overconsumption in the hours following a period of extended fasting. However, meal frequency is highly individual — some people manage hunger better with fewer, larger meals while others do better with more frequent smaller meals. Experimenting with different patterns over 2-week periods to identify which produces lower overall daily hunger provides more useful guidance than any generic recommendation.
Non-Dietary Hunger Management Strategies
Sleep deprivation increases ghrelin (hunger hormone) and decreases leptin (satiety hormone) dramatically — a sleep-deprived person experiences hunger levels equivalent to consuming 300 to 500 fewer calories than they actually did, making deficit adherence physiologically more difficult without any dietary change. Prioritizing 7 to 9 hours of sleep per night during a fat loss phase significantly reduces hunger, making the caloric deficit feel more comfortable at the same intake level. Stress management is equally important: cortisol elevation from chronic stress directly increases appetite (particularly for high-calorie foods) and promotes fat storage — making stress reduction a genuine fat loss strategy rather than a generic wellness recommendation.
The Psychology of Successful Deficit Eating
The behavioral and psychological aspects of maintaining a caloric deficit are as important as the physiological aspects — and substantially underrepresented in most fat loss guidance that focuses almost exclusively on the dietary mechanics. Research from the behavioral psychology of eating identifies several patterns that reliably predict deficit adherence success: all-or-nothing thinking (treating a single off-plan meal as a failed day and abandoning the deficit for the remainder of that day or week) is associated with significantly worse outcomes than flexible restraint (acknowledging the off-plan meal and returning to the plan at the next eating opportunity without guilt or overcompensation). Planning for planned indulgences — scheduling higher-calorie meals or days in advance rather than having them occur reactively — maintains the sense of dietary control that predicts long-term adherence while accommodating the social and emotional dimensions of eating that pure dietary restriction ignores.
The identity-based approach to deficit eating — framing healthy eating as an expression of who you are rather than a set of rules you are following — produces more consistent adherence than willpower-based approaches that treat each food decision as a battle between desire and discipline. “I eat in a way that supports my health and fitness goals” is a more durable motivational frame than “I am not allowed to eat that” — the former comes from internal identity, the latter from external restriction. Building the identity of someone who eats intentionally and healthily — through consistent behavior that reinforces this identity over weeks and months — creates the automatic behavioral tendencies that maintain caloric awareness without continuous active effort.
Practical FAQ
How long should you stay in a caloric deficit?
Most research and practice suggests deficit phases of 8 to 16 weeks followed by a maintenance phase of at least 4 to 8 weeks before resuming restriction. Extended deficits beyond 16 weeks produce compounding metabolic adaptation, hormonal disruption, and psychological restriction fatigue that make additional fat loss increasingly difficult and the quality of life impact increasingly significant. Periodic maintenance phases allow metabolic recovery, hormonal normalization, and psychological restoration that makes subsequent deficit phases more effective and more tolerable.
Why am I not losing weight in a caloric deficit?
The most common reasons: inaccurate calorie tracking (the most frequent cause, resolvable by using a food scale for 2 weeks), metabolic adaptation that has reduced TDEE below the target caloric intake, water retention from dietary sodium or hormonal cycles masking fat loss on the scale (resolvable by tracking weekly averages over 4 weeks), or the deficit is genuinely too small to produce measurable scale changes on a weekly basis. Systematically addressing each of these possibilities — accurate tracking first, then assessing weekly trend data before making dietary adjustments — resolves the vast majority of apparent fat loss stalls.
Can you gain muscle while in a caloric deficit?
Yes, under specific conditions: beginners with significant fat stores, people returning to training after an extended break, and people with high body fat percentages can gain muscle while losing fat — a phenomenon called body recomposition. This simultaneous muscle gain and fat loss becomes progressively less achievable as training experience increases and body fat decreases toward lean levels, but it remains possible for a significant portion of recreational trainees, particularly those who combine high protein intake with consistent resistance training during their deficit phase. For leaner, more experienced trainees, the priority shifts to maximum muscle preservation during fat loss rather than muscle gain, which is the realistic outcome of an optimized deficit approach for this population.
Tracking Progress and Adjusting Your Deficit Over Time
A caloric deficit that produces the expected rate of fat loss in week 1 will often produce slower fat loss by week 6 to 8 due to the metabolic adaptations, reduced body weight (which lowers TDEE), and behavioral drift that affect all extended fat loss phases. Systematic progress tracking and regular deficit recalibration maintain the rate of fat loss through these adaptations and ensure that the deficit remains appropriate as body composition and metabolic rate change.
Weekly Average Weight Tracking
Weighing daily and averaging the 7-day values provides the most reliable assessment of actual weekly fat loss while filtering the noise of daily weight fluctuations. Recording this weekly average in a simple spreadsheet or app and reviewing the month-to-month trend provides the objective progress data needed for deficit adjustment decisions. Expected progress with a well-implemented 500-calorie deficit: 0.4 to 0.6 kg of fat loss per week on average, with individual weeks varying from 0 to 1.2 kg due to water weight fluctuations. A monthly loss of 1.5 to 2.5 kg suggests the deficit is working as intended; significantly less suggests under-eating is not being achieved as intended or metabolic adaptation has reduced TDEE enough to require recalibration.
When and How to Adjust the Deficit
Deficit recalibration is needed when: fat loss has stalled for 2 to 3 consecutive weeks despite consistent adherence to the current caloric target, training performance has declined significantly suggesting energy intake may be too low, or the deficit has been maintained for 12 or more weeks and metabolic adaptation may have significantly reduced TDEE. Adjustment options: reduce daily caloric intake by 100 to 200 calories (a small additional restriction that may restart progress without disproportionate metabolic response), increase NEAT through additional daily walking (which increases TDEE without increasing training load), or implement a diet break — 2 weeks of eating at maintenance calories that partially reverses metabolic adaptation and improves leptin levels before returning to the deficit with renewed effectiveness.
Diet Breaks and Refeeds
Diet breaks (1 to 2 weeks at maintenance) and refeeds (1 to 2 days at maintenance or mild surplus) are evidence-based strategies that improve long-term fat loss outcomes by periodically reversing the metabolic adaptation, leptin reduction, and psychological restriction fatigue that sustained deficits produce. Research shows that people who take planned diet breaks during extended fat loss phases lose more fat over 16 weeks compared to people who maintain continuous restriction — the metabolic and psychological benefits of the maintenance periods more than compensate for the pause in active fat loss. Planning diet breaks into the program from the beginning (rather than taking unplanned breaks driven by adherence failure) maintains the structure and intentionality of the fat loss program through the natural breaks in restriction.
Transitioning Out of a Deficit
The transition from a caloric deficit to maintenance is as important as the deficit itself for long-term body composition outcomes. Rapidly returning to pre-deficit caloric intake produces rapid water weight regain that is often misinterpreted as fat regain, causing panic and immediate return to restriction in a cycle that prevents the stable maintenance most people are seeking. The evidence-based transition protocol is reverse dieting: gradually increasing caloric intake by 50 to 100 calories per week over 4 to 8 weeks, allowing the metabolism to upregulate before adding the full maintenance calories, and monitoring weight weekly to ensure the transition is producing maintenance rather than rapid regain.
Long-Term Maintenance After Fat Loss
Maintaining fat loss after achieving the target is statistically the most challenging phase of the entire fat loss journey — the majority of people who successfully lose fat regain it within 1 to 3 years. The behaviors that predict successful long-term maintenance are well-established in research: regular exercise (the most powerful single predictor, with research from the National Weight Control Registry finding that 90 percent of successful long-term weight maintainers exercise regularly), consistent self-monitoring (weekly weigh-ins and awareness of intake patterns), and the development of eating habits that are genuinely sustainable rather than temporarily tolerated restriction. Building the healthy eating patterns described in this article into permanent lifestyle habits — rather than treating the fat loss phase as a temporary dietary interlude before returning to previous eating patterns — is the foundation of permanent fat loss maintenance.
Deep Dive: The Science of Metabolic Adaptation
Metabolic adaptation — the body’s downregulation of energy expenditure in response to caloric restriction — is the primary reason that extended caloric deficits produce progressively slower fat loss over time. Understanding the specific components of metabolic adaptation allows targeted strategies to minimize its impact and maintain fat loss rate through longer deficit phases.
The four components of metabolic adaptation: (1) Reduced resting metabolic rate from decreased lean mass — the body preferentially catabolizes muscle during a caloric deficit, and each kilogram of muscle lost reduces BMR by approximately 13 calories per day. This is the component most controllable through adequate protein and resistance training. (2) Adaptive thermogenesis — the body reduces thermogenic activity (heat production, fidgeting, organ function) by 100 to 400 calories per day in response to extended restriction. This component is largely involuntary and persists for months after deficit cessation. (3) Reduced NEAT — lower energy availability reduces spontaneous daily movement by 100 to 400 calories without conscious awareness. Taking deliberate steps to maintain NEAT through regular walking partially offsets this component. (4) Reduced exercise energy expenditure — as body weight decreases, the caloric cost of exercise decreases proportionally (moving a lighter body requires less energy). Recalculating TDEE based on reduced body weight and adjusting caloric targets accordingly is the straightforward response to this component.
The cumulative effect of these four components can reduce TDEE by 300 to 600 calories below what TDEE calculation formulas predict after 8 to 12 weeks of restriction — explaining why fat loss slows despite apparent adherence to the original deficit. Accounting for this adaptation through progressive deficit recalibration, planned diet breaks, and consistency in resistance training and protein intake produces better long-term fat loss outcomes than fighting an unchanged deficit against a significantly reduced TDEE.
Practical FAQ
How long should you stay in a caloric deficit?
Most research and practice suggests deficit phases of 8 to 16 weeks followed by a maintenance phase of at least 4 to 8 weeks before resuming restriction. Extended deficits beyond 16 weeks produce compounding metabolic adaptation, hormonal disruption, and psychological restriction fatigue that make additional fat loss increasingly difficult and the quality of life impact increasingly significant. Periodic maintenance phases allow metabolic recovery, hormonal normalization, and psychological restoration that makes subsequent deficit phases more effective and more tolerable.
Why am I not losing weight in a caloric deficit?
The most common reasons: inaccurate calorie tracking (the most frequent cause, resolvable by using a food scale for 2 weeks), metabolic adaptation that has reduced TDEE below the target caloric intake, water retention from dietary sodium or hormonal cycles masking fat loss on the scale (resolvable by tracking weekly averages over 4 weeks), or the deficit is genuinely too small to produce measurable scale changes on a weekly basis. Systematically addressing each of these possibilities — accurate tracking first, then assessing weekly trend data before making dietary adjustments — resolves the vast majority of apparent fat loss stalls.
Can you gain muscle while in a caloric deficit?
Yes, under specific conditions: beginners with significant fat stores, people returning to training after an extended break, and people with high body fat percentages can gain muscle while losing fat — a phenomenon called body recomposition. This simultaneous muscle gain and fat loss becomes progressively less achievable as training experience increases and body fat decreases toward lean levels, but it remains possible for a significant portion of recreational trainees, particularly those who combine high protein intake with consistent resistance training during their deficit phase. For leaner, more experienced trainees, the priority shifts to maximum muscle preservation during fat loss rather than muscle gain, which is the realistic outcome of an optimized deficit approach for this population.




