
How to Fix Rounded Shoulders from Too Much Sitting
⚠️ Disclaimer: The information in this article is for general educational purposes only and does not constitute medical, nutritional, or professional fitness advice. Individual results may vary. Always consult a qualified healthcare professional or certified fitness trainer before starting any new exercise program, changing your diet, or making decisions about injury treatment or recovery. If you experience pain, discomfort, or any unusual symptoms during exercise, stop immediately and seek professional guidance.
Why Sitting All Day Rounds Your Shoulders: The Postural Chain Explained
Rounded shoulders — the forward head, protracted scapulae, internally rotated upper arms posture that has become nearly universal among people who work at computers — is not primarily a posture problem. It is a muscle balance problem that manifests as a posture problem, and the distinction matters enormously for how it is addressed. Years of sitting in a forward-flexed position with arms reaching forward to a keyboard and eyes fixed on a screen at or below eye level produce predictable, progressive changes to the length-tension relationships of the muscles surrounding the shoulder girdle and thoracic spine: some muscles shorten and become hyperactive, others lengthen and become inhibited, and the resulting muscle balance dysfunction is what holds the shoulders in the rounded position regardless of conscious posture efforts. Understanding which muscles are short and which are long is the prerequisite for the targeted stretching and strengthening that actually corrects rounded shoulders — rather than the endless postural reminders and willpower-based “sit up straight” efforts that address the symptom without the underlying cause.
Upper Crossed Syndrome: The Muscle Imbalance Pattern Behind Rounded Shoulders
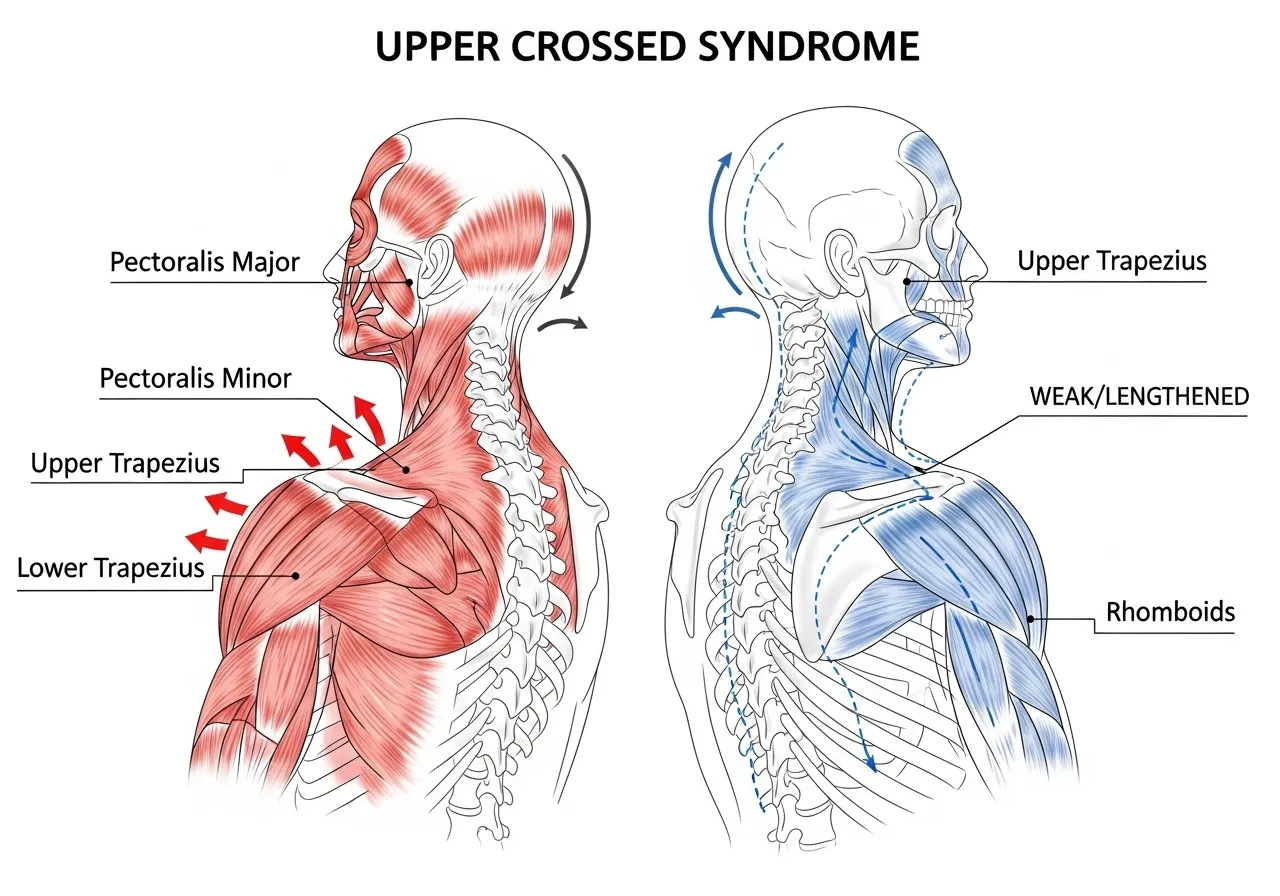
Physical therapist Vladimir Janda described the muscle imbalance pattern underlying rounded shoulders as “upper crossed syndrome” — a crossing pattern of short/overactive and long/inhibited muscles that develops from sustained forward-flexed posture. The short, overactive muscles: pectoralis major and minor (the chest muscles that pull the shoulders forward and internally rotate the arms), anterior deltoid, subscapularis, upper trapezius, levator scapulae, and sternocleidomastoid (neck muscles that become hyperactive to hold the forward-translated head upright). The long, inhibited muscles: lower and middle trapezius (the mid-back muscles that should retract and depress the scapulae), serratus anterior (which should hold the scapula flat against the ribcage), rhomboids, and deep cervical flexors (the front-of-neck muscles inhibited by the tight neck extensors). The “crossed” pattern: short upper traps and pectorals cross with long lower traps and deep neck flexors, creating the characteristic rounded shoulder, elevated shoulder, forward head posture visible in anyone who has spent years at a computer. Research published in the Journal of Orthopaedic and Sports Physical Therapy on upper crossed syndrome consistently finds this specific pattern of muscle dysfunction in desk workers with shoulder pain and postural dysfunction, confirming Janda’s clinical observation across controlled measurement studies.
How Prolonged Sitting Creates These Muscle Changes
Muscle length adaptation occurs through a process called sarcomere remodeling — the addition or removal of sarcomeres (the contractile units within muscle fibers) in response to the habitual length at which the muscle is held. A muscle chronically held in a shortened position (like the pectoralis major held in forward-shoulder position during 8 hours of desk work daily) progressively loses sarcomeres, becoming adaptively shorter and producing resting tension at shorter lengths. A muscle chronically held in a lengthened position (like the middle and lower trapezius held in protracted scapula position) progressively adds sarcomeres, becoming adaptively longer and producing progressively less resting tension at normal lengths — the functional inhibition that makes these muscles feel “weak” even when their strength in isolation is normal. This adaptive shortening and lengthening occurs over months to years of consistent postural exposure — it is not the result of any single long sitting session but the cumulative effect of thousands of hours in the same position. The implication for correction: the adaptations took years to develop and will take months of consistent corrective practice to reverse — not weeks of occasional stretching and posture reminders.
The Thoracic Spine Connection
Rounded shoulders are inseparable from thoracic kyphosis — the excessive forward rounding of the thoracic spine that accompanies and reinforces shoulder protraction. The thoracic spine is the structural foundation of the shoulder girdle: the scapulae sit on the thoracic ribcage, and the angle of the thoracic spine determines the resting position of the scapulae and therefore the starting position of all shoulder movement. Excessive thoracic kyphosis (rounded upper back) mechanically forces the scapulae into protraction — even with optimal shoulder muscle balance, a severely kyphotic thoracic spine will round the shoulders. This means that addressing rounded shoulders requires both restoring the muscle balance that allows correct shoulder position and improving thoracic spine mobility and extension that provides the structural foundation for that position. Thoracic extension mobility work — foam roller thoracic extensions, cat-cow, thoracic rotation — is a necessary component of rounded shoulder correction alongside the pectoral stretching and upper back strengthening that directly addresses the shoulder muscle balance.
How Rounded Shoulders Create Pain and Dysfunction Beyond Posture
The consequences of chronically rounded shoulders extend well beyond appearance — the muscle imbalance and altered shoulder mechanics produce specific pain patterns and movement dysfunctions that affect quality of life and training capacity. Shoulder impingement syndrome — the painful pinching of the supraspinatus tendon and subacromial bursa during shoulder elevation — occurs because rounded shoulders and protracted scapulae reduce the subacromial space through which the rotator cuff tendons pass. Research on subacromial space dimensions finds that scapular protraction reduces the subacromial space by 3–5mm compared to corrected scapular position — a meaningful reduction in the already narrow space that produces the tendon compression causing impingement pain. Neck and upper trap pain — the chronic tension headaches and shoulder tension that plague desk workers — results from the hyperactive upper trapezius and levator scapulae working overtime to hold the forward-translated head upright against gravity, producing the constant high-level activation that eventually creates trigger points and myofascial pain. Reduced overhead range of motion — inability to reach fully overhead without compensatory lumbar extension — results from the combined effects of shortened pectorals pulling the arm into internal rotation and reduced thoracic extension preventing the shoulder elevation that full overhead reach requires. All of these consequences improve with systematic rounded shoulder correction — the posture fix is simultaneously a pain fix and a performance improvement.
Assessment: Identifying Your Specific Rounded Shoulder Pattern
Before beginning a correction program, assessing the specific contributing factors to your rounded shoulder presentation guides exercise prioritization. Simple self-assessment from a side-view photo or mirror: note the position of the earlobe relative to the shoulder — it should be directly above the shoulder in neutral alignment; forward head position (earlobe in front of the shoulder) indicates both rounded shoulders and forward head posture requiring cervical correction alongside shoulder correction. Note whether the shoulders are elevated (shrugged upward, indicating upper trap dominance) or depressed alongside protraction (indicating more pure pectoral tightness). Wall test: stand with back to the wall and try to touch the wall with the back of the head, shoulders, and lower back simultaneously. Inability to get the head to the wall without chin jutting indicates cervical flexor weakness and upper cervical tightness. Inability to get the shoulders flat against the wall without arching the lower back indicates pectoral tightness. These simple assessments identify whether cervical correction should accompany shoulder correction, which muscles are most restricted, and how severe the postural dysfunction has become — guiding the priority and progression of the correction exercises in the following sections.
The Role of Breathing in Rounded Shoulder Posture
The connection between breathing mechanics and rounded shoulders is underappreciated but physiologically significant: the pattern of breathing habitually used during desk work and stress directly influences the postural muscles that determine shoulder position. Chest breathing — shallow breathing that primarily moves the upper chest and accessory breathing muscles (scalenes, sternocleidomastoid, upper trapezius) rather than the diaphragm — keeps the upper trapezius and neck muscles in a state of elevated, near-constant activation that contributes to the hyperactivity of these already-overloaded muscles in the upper crossed syndrome pattern. Diaphragmatic breathing — deep breathing that expands the lower ribcage circumferentially and depresses the diaphragm into the abdomen — activates the diaphragm as the primary breathing muscle, reducing the contribution of the accessory breathing muscles and allowing the upper trapezius and neck muscles to reduce their habitual activation toward normal resting levels. Research on breathing pattern and postural muscle activation finds that chronic chest breathers have significantly higher upper trapezius and scalene resting EMG activity compared to diaphragmatic breathers at equivalent respiratory rates — confirming the direct link between breathing pattern and the postural muscle hyperactivity underlying rounded shoulders. Retraining diaphragmatic breathing — through deliberate daily practice of breathing that expands the lower ribcage and keeps the chest and shoulders relatively still — is therefore a genuine component of rounded shoulder correction, not peripheral relaxation advice.
Why “Sit Up Straight” Doesn’t Work Long-Term
The universal failure of conscious posture reminders — “sit up straight,” “pull your shoulders back,” “chin in” — as a solution to rounded shoulders reflects the fundamental mismatch between the correction they attempt and the actual cause of the problem. Consciously pulling the shoulders back into neutral position requires active muscle contraction against the shortened pectorals and tight anterior shoulder tissues that are pulling them forward — an effort that is fatiguing, uncomfortable, and impossible to sustain across an 8-hour workday of cognitive work that occupies the conscious attention needed to maintain the correction. After minutes or hours, the conscious posture effort fails and the shoulders return to the position of least muscular effort — which, in the upper crossed syndrome pattern, is the rounded position that the short pectorals and inhibited lower traps maintain passively. The sustainable correction approach reverses the muscle balance itself: by stretching the short muscles (reducing the passive forces pulling the shoulders forward) and strengthening the inhibited muscles (increasing the resting tone that holds the shoulders back), the position of least muscular effort becomes the corrected position — and postural correction becomes passive and automatic rather than requiring continuous conscious effort. This is why the exercises in sections 2 and 3 are the actual solution while posture reminders are at best temporary symptomatic management.
The Impact on Athletic Performance: Why Rounded Shoulders Limit Training
Beyond the pain and aesthetics dimensions, rounded shoulders create specific movement limitations that impair athletic performance across a range of training activities. Bench press: internal shoulder rotation from rounded shoulders places the glenohumeral joint in a compromised position for loading — increasing anterior shoulder and pectoral insertion stress while reducing the mechanical efficiency of force transfer through the pressing movement. Overhead press: reduced thoracic extension and shoulder internal rotation prevent the full overhead reach that safe and effective pressing requires, forcing compensatory lumbar hyperextension that increases spinal loading without improving shoulder mechanics. Pull-ups and rows: inhibited lower and middle traps mean that back-dominant pulling movements are performed with excessive upper trap and levator scapulae compensation, reducing the effectiveness of the intended muscle targets while loading the already-overloaded neck and upper shoulder muscles. Squatting and deadlifting: thoracic kyphosis from rounded shoulders reduces the ability to maintain a neutral spine under load, increasing lumbar rounding risk and spinal flexion stress in movements that require thoracic extension for safe mechanics. Correcting rounded shoulders — through the stretching and strengthening protocol in this article — directly improves the shoulder mechanics and thoracic positioning that make all of these movements safer, more mechanically efficient, and more effective.
The physiology of rounded shoulder development — adaptive muscle shortening, inhibition of opposing muscles, thoracic kyphosis, and breathing pattern reinforcement — creates an interconnected dysfunction that requires a systematic, multi-component correction approach. The stretching, strengthening, habit, and awareness practices that follow address each component of this system. The understanding of why rounded shoulders develop — adaptive shortening through sustained positioning, inhibition of opposing muscles, thoracic kyphosis as structural foundation, and breathing pattern reinforcement — transforms the correction approach from symptom management to root cause intervention. Every exercise and habit in this program targets a specific mechanism in this causal chain, and the comprehensive approach that addresses all mechanisms simultaneously produces faster and more lasting correction than any single-element approach. The years invested in desk work and device use that created the rounded shoulder pattern are not wasted — they represent the professional and personal productivity that modern life demands. But the postural cost of that investment is real, measurable, and correctable. The 15 minutes per day required to systematically correct rounded shoulders is a return investment that pays compound returns in comfort, performance, and long-term joint health across decades of continued active life.

The Best Stretches to Open Your Chest and Release Rounded Shoulder Tension
Stretching the short, overactive muscles of the anterior shoulder complex — the pectorals, anterior deltoid, subscapularis, and upper trapezius — is the first phase of rounded shoulder correction because these shortened tissues are the primary passive forces holding the shoulder girdle in the rounded position. Until these muscles are progressively lengthened and their resting tension reduced, strengthening the opposing muscles is fighting against a mechanical disadvantage: the rhomboids and lower trapezius cannot pull the scapulae into retraction against significantly shortened pectorals any more than a weak rope can overcome a tight spring. Stretching comes first, sustained stretching over weeks produces the sarcomere remodeling that genuinely lengthens these tissues, and the strengthening that follows then has a corrected mechanical environment in which to develop the muscle balance that holds the correction permanently.
Doorway Pectoral Stretch: The Foundation Chest Opener
The doorway pectoral stretch is the most accessible and most consistently effective pectoral major stretch, requiring only a doorframe and the correct technique that distinguishes a genuine pectoral stretch from a mere shoulder position change. Stand in a doorway with one arm bent at 90 degrees, forearm resting on the doorframe at shoulder height, and step forward with the same-side foot until you feel a stretch across the chest and anterior shoulder — not a pinch at the shoulder joint, which indicates impingement rather than tissue stretch. Hold 30–45 seconds, perform 3 repetitions per side, 2–3 times daily. Three arm positions stretch different portions of the pectoral major: arm at shoulder height (middle fibers, the most commonly tight), arm slightly above shoulder height (lower fibers), and arm slightly below shoulder height (upper fibers). Performing the stretch at all three positions across the day provides comprehensive pectoral major lengthening. The common error that makes this stretch ineffective: allowing the ribcage to rotate with the shoulder rather than keeping the torso squared to the doorway. Ribcage rotation allows the pectoral to lengthen by moving the origin (ribcage) rather than the insertion (humerus) — maintaining a squared torso ensures the stretch lengthens the muscle fibers rather than rotating the spine.
Foam Roller Thoracic Extension: Opening the Kyphotic Spine
The thoracic spine extension that rounded shoulders compress requires deliberate mobilization through a counter-movement that directly addresses the stiffened thoracic segments. Place a foam roller perpendicular to the spine at the mid-thoracic region (approximately between the shoulder blades), support the head with hands interlaced behind it, and allow the thoracic spine to extend over the roller — letting gravity gradually increase thoracic extension over 30–60 seconds at each spinal level. Move the roller upward by shifting the body, addressing 3–4 different vertebral levels from mid-thoracic to upper thoracic. This passive mobilization progressively restores thoracic extension range of motion that sustained kyphotic positioning has reduced, creating the spinal foundation that allows the scapulae to retract toward the corrected position. Frequency: daily, or twice daily for those with significant thoracic stiffness. Avoid the lumbar spine and neck — the roller should contact only the thoracic region between the bottom of the shoulder blades and the base of the neck. Initial sessions may be uncomfortable as stiff thoracic segments mobilize; this discomfort diminishes with consistent practice as mobility is progressively restored.
Pectoralis Minor Stretch: The Deep Anterior Shoulder Opener
The pectoralis minor — the deeper, smaller chest muscle that attaches to the coracoid process of the scapula and the 3rd–5th ribs — is often overlooked in shoulder posture correction because it is hidden beneath the larger pectoralis major, but its tightness directly tilts the scapula anteriorly (tipping the coracoid forward and the inferior scapular angle away from the ribcage) in a way that limits scapular upward rotation and reduces subacromial space. Stretching the pectoralis minor specifically: lie face-up with a rolled towel along the spine from tailbone to head (creating a gentle spinal extension support), arms relaxed at the sides, and allow the shoulders to relax toward the floor under gravity for 3–5 minutes. The gentle passive external rotation and scapular retraction this position encourages directly addresses pectoralis minor tightness and anterior scapular tilt. Research on pectoralis minor length and shoulder posture published in the PubMed literature identifies pectoralis minor shortness as a primary driver of scapular anterior tilt that is distinct from pectoralis major tightness and requires its own specific addressing.
Upper Trapezius and Levator Scapulae Neck Stretches
The upper trapezius and levator scapulae — both hyperactive in the upper crossed syndrome pattern from their constant effort to support the forward-translated head — develop significant muscle tension and trigger points that contribute to neck pain, tension headaches, and the shoulder elevation pattern that accompanies rounded shoulders. Upper trapezius stretch: sitting or standing, gently side-bend the head (right ear toward right shoulder) while reaching the left hand down toward the floor — the gentle traction on the left upper trapezius combined with the side-bend creates a gentle lengthening stretch. Hold 30 seconds per side, 3 repetitions. Levator scapulae stretch: rotate the head to 45 degrees (looking toward the armpit), then gently nod the chin toward the chest — this specific rotation-flexion combination targets the levator scapulae fibers that run at this angle. Hold 30 seconds per side, 3 repetitions. Both stretches should produce a comfortable, mild tension sensation in the neck and upper shoulder region — not sharp pain or neurological symptoms (tingling, numbness, weakness). Frequency: 2–3 times daily, particularly after periods of sustained desk work that load these tissues.
Sleeper Stretch: Internal Shoulder Rotation Release
The sleeper stretch addresses the posterior shoulder capsule and internal rotator muscles (subscapularis, anterior deltoid) that are shortened in chronically rounded shoulders. Lie on the side of the arm being stretched, upper arm at 90 degrees from the torso, elbow bent to 90 degrees. Using the other hand, gently press the forearm toward the floor (into external rotation) until a stretch is felt at the back of the shoulder or posterior arm. Hold 30 seconds, perform 3 repetitions per side. The sleeper stretch is particularly important for athletes who bench press heavily — the internal rotation stress of heavy pressing further shortens the already-tight subscapularis and anterior capsule that sitting promotes, and neglecting this stretch contributes to the “bench presser’s shoulder” impingement pattern common in gym athletes who press heavily without addressing the internal rotation asymmetry it promotes.
Cat-Cow and Thoracic Rotation: Mobility Drills for the Kyphotic Spine
The thoracic spine requires not just passive extension mobilization (from the foam roller) but active mobility exercises that develop controlled movement through the restored range. Cat-cow: on hands and knees, alternate between spinal flexion (arching the back toward the ceiling, chin to chest) and extension (dipping the belly toward the floor, head and tailbone up) — focus on the thoracic segment producing the maximum movement range while limiting compensatory motion from the lumbar spine and neck. 10–15 repetitions, moving slowly and breathing with each direction. Thoracic rotation: seated in a chair, cross the arms over the chest and rotate the torso to each side — isolating thoracic rotation by maintaining the lower back against the chair back and keeping the pelvis stationary. 10 rotations each direction, feeling the stretch through the thoracic facets and intercostal spaces. These active mobility drills translate the passive range gained from foam rolling into usable, active movement control that the nervous system can access during training and daily activity — converting passive range into active mobility that the postural correction can utilize.
Stretching Protocol: Frequency, Duration, and Sequencing
The stretching component of rounded shoulder correction requires higher frequency than most people apply to produce the tissue length changes that are visible on the months-long timeline of sarcomere remodeling. Research on static stretching duration and frequency for muscle length change finds that gains in flexibility are dose-dependent — more total weekly stretching time produces more length change — with a minimum of 2 minutes of cumulative stretch time per muscle per week required for measurable adaptation. For the pectoral major and minor: three 45-second holds performed twice daily provides 9 minutes of weekly cumulative stretch time — above the minimum effective dose. Optimal stretching timing: after warming the tissues with light movement or a warm shower (warm tissue stretches more safely and produces better acute length increases than cold tissue), and never immediately before a strength session (acute static stretching reduces muscle force production for 30–60 minutes post-stretch — perform the strength exercises first, then stretch the tight anterior muscles). The stretching protocol requires 10–15 minutes daily to execute completely — a modest time investment relative to the chronic postural dysfunction it corrects across consistent weeks of practice.
Self-Myofascial Release: Foam Rolling for Rounded Shoulder Correction
Self-myofascial release — using a foam roller, lacrosse ball, or massage stick to apply sustained pressure to tight muscles — complements stretching by addressing the trigger points and myofascial adhesions that limit muscle extensibility beyond what passive stretching alone can reach. For rounded shoulder correction, the highest-priority self-myofascial release targets are the upper trapezius (roll from the base of the skull along the top of the shoulder to the acromioclavicular joint, pausing on tender points for 20–30 seconds), the pectoral major (place a lacrosse ball between the pectoral and a wall, leaning body weight into it and moving slowly to find tender areas), and the thoracic spine extensors (foam roller placed along the thoracic spine for the extension mobilization described above). Self-myofascial release works by mechanoreceptor stimulation that temporarily reduces muscle tone and allows greater tissue extensibility during the subsequent stretch — the combination of SMR followed immediately by the corresponding static stretch produces greater acute flexibility improvements than either technique alone. The sequence: SMR for 60–90 seconds on the target tissue, immediately followed by the static stretch for 2–3 × 45-second holds, captures the acute extensibility benefit that SMR creates before muscle tone normalizes. Daily SMR combined with daily stretching of the tight anterior shoulder tissues is the most effective conservative approach to accelerating the tissue lengthening that is the rate-limiting step in rounded shoulder correction.
Breathing Retraining: Diaphragmatic Practice for Postural Change
Restoring diaphragmatic breathing as the primary breathing pattern reduces the chronic upper trapezius and accessory breathing muscle activation that perpetuates the muscle tension component of upper crossed syndrome. Diaphragmatic breathing practice: lie on the back with knees bent, one hand on the chest and one on the lower abdomen. Inhale slowly through the nose, directing the breath to expand the lower ribcage and lift the abdominal hand — the chest hand should remain relatively still. Exhale slowly and completely, allowing the abdomen to fall. Practice 10 deliberate diaphragmatic breaths 3 times daily, and progressively carry the pattern into seated and standing positions as the movement becomes more automatic. Research on breathing retraining programs for postural dysfunction finds significant reductions in upper trapezius resting EMG activity after 4 weeks of consistent diaphragmatic breathing practice — confirming the direct link between breathing pattern and the postural muscle hyperactivity underlying rounded shoulders. The breathing retraining takes 5 minutes per session and can be performed during typically unproductive times (waiting for coffee to brew, sitting in traffic, during routine meetings) — the low time cost and broad physiological benefits make it among the highest return-on-investment components of the rounded shoulder correction protocol.
The stretching and mobility practices in this section create the prerequisite tissue extensibility and joint mobility that allow the strengthening exercises in the next section to build muscle balance in the corrected mechanical environment — making the two phases complementary and sequentially dependent rather than interchangeable alternatives. The stretching practices in this section are most effective when applied with the frequency and duration that tissue adaptation requires — not as occasional additions to training when shoulder discomfort prompts attention, but as daily, consistent practices that accumulate the cumulative stretch time that sarcomere remodeling demands across the weeks of consistent application that produce measurable tissue length change.

Strengthening Exercises That Permanently Fix Rounded Shoulders
Stretching the short anterior muscles removes the passive forces pulling the shoulders forward; strengthening the long, inhibited posterior muscles provides the active forces that hold them back. Both are required for lasting correction — stretching alone produces temporary improvement that regresses when the muscles return to their shortened length without the opposing strength to maintain the corrected position, and strengthening alone fights the mechanical disadvantage of tight pectorals. The exercises in this section target the specific muscles that are inhibited in upper crossed syndrome: lower and middle trapezius, rhomboids, serratus anterior, and the external rotators. They are organized from most accessible (appropriate for anyone) to most demanding (appropriate for intermediate trainees with baseline strength).
Band Pull-Apart: The Essential Shoulder Retractor
The band pull-apart is the single most important exercise for rounded shoulder correction — it specifically activates the lower and middle trapezius and rhomboids in the scapular retraction movement that directly opposes shoulder protraction, and it can be performed anywhere with a resistance band. Hold a resistance band at shoulder width with arms extended in front, palms down. Pull the band apart by moving both arms outward until the band touches the chest, feeling the scapulae retract and the mid-back muscles engage, then slowly return. The quality cues that make this exercise therapeutically effective: keep the arms at or slightly below shoulder height (not elevated, which shifts activation to the upper trapezius), actively pull the shoulder blades together and downward (not just backward — the lower trap component requires the depression element), and maintain a neutral spine without arching the lower back in compensation. Sets/reps: 3 sets of 15–20 reps, 3–4 times per week. Light band resistance that allows full range with controlled technique is more valuable than heavy bands that compromise range and allow upper trap substitution. Progression: increase band resistance, vary the arm height (slightly high = more upper mid-trap emphasis, slightly low = more lower trap emphasis), or add a 2-second hold at the end range of retraction.
Face Pull: The Rotator Cuff and Lower Trap Combination
The face pull — performed with a cable machine rope attachment or resistance band anchored at face height — is the second most important exercise for rounded shoulder correction because it simultaneously trains external rotation (addressing the internal rotation bias of rounded shoulders) and scapular retraction (addressing the protraction) in one movement. At a cable machine with rope attachment at face height, grip the rope and pull toward the face while simultaneously externally rotating — splitting the rope apart as the elbows flare outward and the hands end up beside the ears at the completion of the movement. The combined external rotation and retraction at the finish position is the direct opposite of the internally rotated, protracted shoulder of rounded shoulder posture. Sets/reps: 3 sets of 15–20 reps. Common error: pulling with the arms without adequate external rotation, producing a rowing motion that trains biceps and mid-trap without the external rotation component that specifically addresses the rotational component of rounded shoulders. Research consistently identifies face pulls as one of the highest-activating exercises for the infraspinatus and teres minor — the primary external rotators inhibited in rounded shoulder posture — alongside their lower and middle trapezius activation.
Prone Y, T, W Raises: Direct Lower Trapezius Isolation
The prone Y-T-W sequence — performed lying face down on a bench or floor, or inclined on an adjustable bench — directly targets the lower trapezius in its primary function of scapular depression and upward rotation, the movement that is most specifically inhibited in upper crossed syndrome. Y raise: arms at approximately 135 degrees from the torso (Y position), thumbs up, lift the arms while retracting and depressing the scapulae — feeling the lower trapezius between the spine and the lower tips of the shoulder blades contract. T raise: arms straight out to the sides at 90 degrees, same scapular retraction and depression cue. W raise: elbows bent to 90 degrees, arms forming a W shape, externally rotate and retract simultaneously. All three can be performed with no weight initially (the resistance of the arm’s weight is sufficient for many people with significant lower trap inhibition), progressing to light dumbbells (1–3kg). Sets/reps: 2–3 sets of 10–12 reps of each position. The Y, T, and W positions collectively train the lower trapezius through its full functional range — the varying arm angles challenge the muscle at different points in its length-tension curve, developing balanced strength throughout the range of motion that functional activities require.
Seated Row: The Compound Posterior Chain Exercise
The seated cable row (or banded row) provides the compound strengthening stimulus for the full posterior shoulder complex — rhomboids, middle trapezius, lower trapezius, and rear deltoid — that the isolation exercises complement but do not fully develop. Seated at a cable machine with feet on the platform, grip the handle and row toward the lower abdomen, leading with the elbows and squeezing the shoulder blades together at the completion of the movement. The critical technique point for rounded shoulder correction: retract the scapulae first, then pull with the arms — initiating the movement with scapular retraction ensures the rhomboids and traps are the primary movers rather than allowing the arms to drive a purely arm-dominant rowing pattern that minimizes the back contribution. Sets/reps: 3 sets of 10–12 reps, progressing weight as technique is maintained. Tempo: slow eccentric (3–4 seconds) returning the weight to emphasize the eccentric strength of the retractors — the controlled lengthening phase builds functional strength through the range of motion that matters most for postural correction.
Serratus Anterior Activation: The Forgotten Scapular Stabilizer
The serratus anterior — the finger-like muscle running from the medial scapular border to the lateral ribcage — holds the medial scapular border against the ribcage and provides the upward rotation force that positions the scapula optimally during shoulder elevation. Its inhibition in rounded shoulders contributes to the medial scapular winging that reduces shoulder joint stability and shoulder elevation range. Serratus anterior activation exercises: wall push-up plus — perform a push-up against a wall, then at the top of the movement, add a final push that protracts the scapula and rounds the upper back (the “plus” phase) — this scapular protraction against resistance directly activates the serratus anterior in its primary function. Scapular push-up: in a push-up position without bending the elbows, protract and retract the scapulae by spreading and pinching the shoulder blades — the protraction phase activates the serratus while the retraction phase engages the rhomboids, making this a balanced activation exercise for both. Sets/reps: 2–3 sets of 10–15 reps of each variation.
External Rotation Exercises: Correcting Humeral Internal Rotation
The chronic internal rotation of the humerus (upper arm bone) in rounded shoulder posture produces shortened internal rotators (subscapularis, pectoralis major, anterior deltoid) and inhibited external rotators (infraspinatus, teres minor). Strengthening the external rotators directly corrects this rotational imbalance. Banded or cable external rotation: standing with the elbow at 90 degrees and held against the side, grip the band or cable handle and rotate the forearm outward against resistance — keeping the elbow anchored against the ribcage throughout. 3 sets of 15 reps per side, with light resistance that allows full external rotation range. Side-lying dumbbell external rotation: lying on the side, elbow bent to 90 degrees, rotate the dumbbell upward against gravity — the most direct external rotator strengthening exercise. 3 sets of 12–15 reps with light dumbbells (2–5kg). These exercises have relatively low loading requirements — the infraspinatus and teres minor are small muscles that are easily overloaded with heavy weight — and are most beneficial at moderate weights with full range of motion and deliberate slow tempo.
Chin Tuck: Correcting Forward Head Posture Alongside Rounded Shoulders
Forward head posture — the anterior translation of the head relative to the shoulders that accompanies and reinforces rounded shoulder posture — requires its own targeted correction alongside the shoulder exercises. The chin tuck exercise directly strengthens the deep cervical flexors (longus colli, longus capitis) that are inhibited in forward head posture, while simultaneously stretching the suboccipital extensors that are shortened. Sitting or standing with the spine in neutral, gently draw the chin straight back (not downward — the movement is retraction, not flexion, creating a “double chin” position), hold 5 seconds, release. 10–15 repetitions, 3 times daily. The chin tuck feels unusual initially — most people with chronic forward head posture experience the retracted position as abnormal because their nervous system has normalized the forward position — but with consistent practice the neutral cervical alignment progressively becomes the automatic resting position. Research from the American Physical Therapy Association’s clinical guidelines identifies chin tuck exercise as the most evidence-supported intervention for forward head posture correction, with consistent improvement in cervical muscle balance and neck pain reduction across 8–12 weeks of regular practice.
How Pressing and Pulling Balance Affects Shoulder Posture
For athletes who perform resistance training, the ratio of pressing to pulling exercises in the training program directly contributes to or corrects rounded shoulder posture. Most recreational training programs are significantly press-dominant — bench press, overhead press, and their variations receive primary training emphasis while rowing and pulling exercises are secondary or neglected. Each pressing repetition loads the pectorals and anterior deltoid in the shortened position, reinforcing the adaptive shortening that promotes rounded shoulders. Each pulling repetition loads the rhomboids, middle and lower trapezius, and rear deltoid in contraction — the muscles that correct rounded shoulders. A pressing-to-pulling volume ratio of 1:1.5 to 1:2 (significantly more pulling than pressing volume) is recommended for athletes with existing rounded shoulder posture — the extra pulling volume over time progressively restores the posterior shoulder strength that corrects the protraction pattern. Specific exercise substitutions for improving this ratio: replace one press day with an additional pull day, add face pulls and band pull-aparts as daily warm-up regardless of the main session’s focus, and ensure that every pressing session is balanced with equal or greater pulling volume on the same or following day. The training program is therefore a daily intervention in rounded shoulder posture correction or perpetuation — not an activity separate from the postural problem but a primary driver of it in either direction.
Progressive Overload for Postural Correction Exercises
The strengthening exercises for rounded shoulder correction follow the same progressive overload principle as any resistance training — the muscles develop in response to progressively increasing stimulus, and exercises that remain at a fixed difficulty level eventually produce no further strength or muscle adaptations. The progression sequence for the key exercises: band pull-apart progresses from light band to medium to heavy band over 8–12 weeks; face pulls progress from 5kg to 20kg+ on the cable machine; prone Y-T-W progresses from no weight to 1kg to 3kg dumbbells; seated row progresses in standard resistance training fashion with load increments of 2.5–5kg when technique is consistently clean. The critical distinction from the early phases of rehab-focused strengthening: as pain resolves and movement quality improves, the exercises should be treated as genuine strength training rather than gentle corrective exercise — progressive load increases that produce the hypertrophic adaptations of the lower and middle trapezius and rhomboids are what creates the lasting muscle balance that holds the corrected posture automatically rather than requiring constant conscious effort.
The strengthening phase, applied consistently after the stretching phase has created adequate anterior tissue extensibility, is what converts temporary postural improvement into permanent structural correction. The strengthening exercises for rounded shoulder correction become most effective when progressed to genuine therapeutic resistance training intensity — not the minimal-resistance, high-repetition approach that is appropriate only for the initial activation phase, but the progressive loading that produces the hypertrophic adaptations in the lower and middle trapezius and rhomboids that permanently shift the muscle balance equation away from the anterior dominance of rounded shoulders.

Daily Habits, Workstation Setup, and Postural Correction Routines
The exercises and stretches in sections 2 and 3 will correct rounded shoulders on the hours they are performed but will be systematically undermined if the remaining 8–10 hours of the workday are spent in the same forward-flexed, internally rotated position that created the problem in the first place. Lasting postural correction requires both the targeted corrective exercises and modification of the daily postural environment — the workstation setup, movement habits, and postural breaks that determine the total exposure to rounded shoulder positioning across the 16 waking hours that the daily corrective session must overcome. This section addresses the environmental and habitual factors that either support or undermine the corrective work being done in dedicated exercise sessions.
Ergonomic Workstation Setup for Rounded Shoulder Prevention
The workstation is the physical environment that determines the postural loading pattern for 8+ hours daily — its setup directly determines how much forward shoulder positioning is required by the work tasks it supports, making ergonomic optimization the highest-leverage environmental intervention for desk workers with rounded shoulders. Monitor height and distance: the top of the monitor should be at or slightly below eye level (not below — looking down at a monitor throughout the day flexes the cervical spine into the forward head position that accompanies rounded shoulders), positioned at approximately arm’s length. A monitor that is too low — including laptop screens used without a stand — produces the most common workstation posture error, forcing the head and neck into sustained flexion that directly loads the upper trapezius and levator scapulae in their hyperactive pattern. Keyboard and mouse positioning: the keyboard should be positioned so the elbows are at approximately 90 degrees when typing, with the arms close to the sides rather than reaching forward — reaching forward to a distant keyboard maintains the shoulder protraction that stretching is trying to reverse. Chair height and lumbar support: the chair should be set so the thighs are approximately horizontal or slightly declined (front lower than back), with feet flat on the floor, and a lumbar support that maintains the natural lumbar curve reduces the tendency for the entire spine to round when sitting fatigue occurs.
Postural Microbreaks: Movement Every 30 Minutes
The adaptive muscle length changes that produce rounded shoulders occur through sustained, static positioning — the continuous maintenance of the same shoulder protraction angle for hours at a time. Interrupting this sustained positioning with brief movement breaks every 20–30 minutes prevents the sustained loading that drives adaptive shortening while also providing the circulation and joint lubrication that sustained static posture denies. The microbreak protocol requires only 60–90 seconds every 30 minutes: stand up, perform 10 band pull-aparts or doorway stretches if accessible, or simply perform 5 shoulder rolls and 5 chest opening movements (arms swept back behind the body to the maximum comfortable range). Research on movement breaks and musculoskeletal health in office workers finds that 2-minute movement breaks every 30 minutes produce significant reductions in neck and shoulder discomfort, muscle tension, and postural deviation compared to continuous sitting — with benefits appearing within the first week of consistent implementation. The practical challenge is remembering the breaks against the absorbing nature of knowledge work; solutions include phone reminders, computer desktop reminder apps (Stand Up! for Mac, Break Reminder for Windows), and wearable devices that vibrate at set intervals to prompt movement.
Standing Desk Usage: Benefits and Correct Implementation
Standing desks have become a popular workstation alternative for desk workers concerned about the health consequences of prolonged sitting, but their benefit for rounded shoulders specifically depends on how they are used. Standing at a desk can reduce hip flexor shortening and the lumbar flexion that accompanies sitting — positive effects for overall postural health. However, standing without deliberate attention to shoulder position and monitor height produces the same or worse rounded shoulder pattern as sitting — people who stand at desks without monitor stands still look down at screens, reach forward to keyboards, and internally rotate their shoulders in exactly the same pattern as sitting workers. The correct standing desk implementation for rounded shoulder correction: monitor at true eye level (may require a separate monitor stand even with an adjustable desk), keyboard at elbow height when standing, anti-fatigue mat for comfort, and alternating between sitting and standing every 30–60 minutes rather than standing exclusively (prolonged static standing produces its own fatigue and postural deviation). Standing is only beneficial for rounded shoulders if the monitor and keyboard position is corrected alongside the change from seated to standing — the height change alone without position correction simply places the same problematic postural loading at a different elevation.
Sleeping Position and Pillow Selection for Shoulder Posture
The 7–9 hours spent sleeping represent a significant proportion of the daily postural environment — and sleeping positions that place the shoulder in sustained protraction and internal rotation during the night actively undermine the daytime corrective work. Sleeping on the side with the shoulder rolled forward (the most common side-sleeping position) places the downside shoulder in sustained protraction and the spine in lateral flexion for hours, directly reinforcing the muscle length adaptations that daytime corrective exercises are trying to reverse. Optimizing sleep position for rounded shoulder correction: back sleeping with arms at the sides (or a pillow under the knees for lumbar comfort) is the ideal position — it places both shoulders in a neutral, gravity-assisted retracted position for the duration of sleep, passively supporting the correction rather than undermining it. For side sleepers who cannot comfortably sleep on their back: placing a pillow between the arms (hugging a body pillow) prevents the shoulder from rolling fully forward into maximum protraction. Pillow height: for back sleepers, a single pillow that maintains the cervical spine in neutral (not elevated enough to push the head into forward flexion) supports the forward head correction alongside the shoulder position. For side sleepers, a pillow that fills the space between the shoulder and the ear (keeping the cervical spine straight rather than laterally flexed) reduces the neck muscle stress of unsupported side sleeping.
Phone and Tablet Use: The “Tech Neck” Companion Problem
Smartphone and tablet use has added a second major driver of forward head and rounded shoulder posture alongside desk work — the sustained downward gaze and forward head tilt of phone use loads the cervical spine with 4–5 times the force of neutral head position (the head weighing effectively 27kg at 60 degrees of forward tilt versus 5kg in neutral), producing accelerated upper crossed syndrome development beyond the desk work contribution alone. Strategies for reducing phone-related postural loading: hold the phone at eye level rather than looking down at it (awkward initially but significantly reduces the cervical loading that produces forward head posture), use voice control for frequent tasks that require repeated screen interaction, limit prolonged phone use to positions that support the arm (lying on the back with the phone held above the face, or using a phone stand that positions the screen at eye level). These adjustments are individually small but collectively meaningful when applied across the hours of daily phone use that have become typical in contemporary life.
The Daily Postural Correction Routine: 15 Minutes That Change Everything
Consolidating the stretching, strengthening, and mobility components of rounded shoulder correction into a structured daily routine ensures consistent execution within a realistic time investment. The complete 15-minute daily routine: morning (8 minutes) — doorway pectoral stretch 3 × 45 seconds each side (3 min), foam roller thoracic extension for 3 levels (2 min), cat-cow 10 repetitions (1 min), chin tucks 15 repetitions (1 min), diaphragmatic breathing 10 breaths (1 min). Post-work or training (7 minutes) — band pull-aparts 3 × 20 (2 min), face pulls 3 × 15 (2 min), prone Y-T-W 2 × 10 each (2 min), sleeper stretch 2 × 30 seconds each side (1 min). This routine addresses the full correction system — tissue extensibility through the morning stretches, thoracic mobility through the foam roller and cat-cow, neuromuscular activation through the chin tucks, and posterior shoulder strengthening through the band exercises — in a total of 15 minutes that can be split between morning and evening or performed as a complete session. The consistency of a daily routine — rather than the episodic “whenever I remember” approach that fails to produce the sustained tissue-length changes required for permanent correction — is what actually fixes rounded shoulders across the weeks and months the correction requires.
Postural Awareness Training: Building the Internal Feedback System
Beyond the environmental modifications and movement breaks, developing the internal postural awareness that detects shoulder protraction and automatically corrects it before it becomes sustained loading requires deliberate training of the proprioceptive feedback that most people with rounded shoulders have lost. Postural awareness exercises: hourly shoulder position checks (setting a phone alarm once per hour as a reminder to assess shoulder position — where are the shoulders right now? What is the head position relative to the shoulders?) train the metacognitive awareness that eventually becomes habitual monitoring without reminder. Mirror and video feedback: periodically working at a standing desk or exercising in front of a mirror develops visual feedback for shoulder position that supplements the impaired proprioceptive feedback that has normalized the rounded position as “straight.” Body scan practice: the same mindfulness-based body scanning used in meditation — systematically directing attention through the body from head to toe — applied specifically to shoulder and neck position during otherwise routine activities (waiting in lines, commuting, sitting in meetings) develops the continuous low-level postural monitoring that reduces the unconscious drift toward protraction that occurs when attention is absorbed by cognitive tasks. These awareness practices are the bridge between the deliberate exercise sessions and the automatic postural correction that represents the long-term goal of the correction program.
Children and Teenagers: Early Intervention for Screen-Related Posture
The rounded shoulder epidemic is accelerating in younger populations as childhood screen time increases — children who spend 4–8 hours daily on devices during school and leisure time are developing the upper crossed syndrome patterns in their teenage years that previous generations did not encounter until their 30s and 40s. Early intervention is significantly more effective than later correction because the adaptive tissue length changes are less established and more rapidly reversible in growing bodies, and the movement habits that support corrected posture are easier to establish before the years-long reinforcement of poor habits makes them deeply ingrained. For children and teenagers: age-appropriate strength and stretching education (body-weight rows, resistance band pull-aparts, doorway stretches), mandatory outdoor play and physical activity that provides natural movement variation that sedentary screen time eliminates, screen positioning at eye level rather than in the lap, and the modelling of good postural habits by adults in the household — the most powerful postural intervention for children being the postural behavior they observe most often in the adults around them.
The daily habits and environmental modifications in this section determine whether the corrective exercises have a fighting chance against the postural forces of modern sedentary life — without them, even perfectly executed exercises are overwhelmed by the volume and consistency of the daily postural loading that produces and perpetuates rounded shoulders. The cumulative effect of workstation optimization, movement breaks, corrected sleep position, and postural awareness practice reduces the total daily rounded shoulder exposure from 8–10 hours to 2–3 hours — a reduction that makes the corrective exercise session’s effect lasting rather than immediately overwhelmed by the volume of postural loading it must overcome.

How Long It Takes to Fix Rounded Shoulders, Common Mistakes, and FAQs
One of the most important expectations to set correctly at the beginning of a rounded shoulder correction program is the timeline — the realistic duration that consistent, correctly applied corrective practice requires before permanent structural change is established. Most people who attempt rounded shoulder correction expect visible improvement within days and lasting change within weeks, and abandon the program when these expectations are not met. The reality of the tissue adaptation timeline — sarcomere remodeling, muscle balance restoration, and neuromuscular reprogramming — requires months of consistent practice for meaningful correction and years for complete resolution of long-established dysfunction. Understanding this timeline not as discouragement but as accurate planning converts the rounded shoulder correction program from a short-term fix attempt into the sustainable long-term practice that actually produces the desired outcome.
The Realistic Timeline for Rounded Shoulder Correction
Rounded shoulder correction follows a predictable but slow timeline that reflects the physiology of adaptive muscle length change and muscle balance restoration. Week 1–4: acute tissue response — reduced muscle tension and trigger point activity from consistent stretching and SMR, improved subjective shoulder comfort, first signs of increased thoracic extension mobility. Months 2–3: measurable range improvements — pectoral flexibility visibly improving (wall test and doorway stretch depth increasing), postural position measurably improved at the end of stretching sessions, initial strength gains in the band pull-apart and face pull. Months 4–6: functional postural improvement — the corrected shoulder position beginning to be maintained more automatically during sedentary work, reduced trigger point recurrence in the upper trapezius and levator scapulae, shoulder discomfort during pressing movements decreasing as external rotation improves. Months 6–12: structural consolidation — the corrected posture becoming the resting default rather than a consciously maintained position, posterior shoulder strength sufficient to maintain correction against daily postural loads, thoracic extension mobility substantially restored. Years 1–2+: complete resolution — for individuals with severe, long-established rounded shoulders, full resolution of all adaptive tissue changes and full automatic postural correction may require 1–2 years of consistent practice. This timeline is not discouraging when framed correctly: the improvements are progressive and visible from the beginning of the program, even if complete correction is a long-term process.
Common Mistakes That Prevent Rounded Shoulder Correction
Several predictable mistakes consistently prevent rounded shoulder correction programs from producing their intended outcomes. Stretching without strengthening: addressing only the tight anterior muscles without building the strength of the inhibited posterior muscles produces temporary improvement — the pectoral lengthens slightly from stretching, but without lower trap and rhomboid strength to hold the corrected position, the shoulder drifts back to protraction as soon as the stretch session ends. Strengthening without stretching: building strength in a mechanically disadvantaged position against shortened pectorals produces strength adaptations but minimal postural change — the posterior muscles become stronger at holding the protracted position more firmly rather than being able to pull against the shortened anterior tissues into corrected position. Performing only 2–3 repetitions of each stretch rather than the minimum effective dose (3 sets of 45+ seconds): research on static stretching consistently finds that flexibility adaptations require adequate cumulative stretch time — short, infrequent stretches produce minimal tissue length change. Treating the correction program as a temporary intervention rather than a permanent training component: the rounded shoulder tendency persists as long as the lifestyle that created it (prolonged desk work, pressing-dominant training, phone use) continues — the correction exercises must become a permanent component of the movement diet rather than a temporary program completed once and discontinued.
When to See a Physical Therapist
Self-managed rounded shoulder correction is appropriate and effective for most people with postural dysfunction without significant pain or movement limitation. Professional physical therapy evaluation is recommended when: shoulder pain is significant and persistent (preventing comfortable sleep, limiting daily activity, or failing to improve with 6–8 weeks of self-managed corrective exercise); neurological symptoms (numbness, tingling, or weakness in the arm or hand) accompany the shoulder symptoms (suggesting cervical nerve root or brachial plexus involvement requiring differential diagnosis); the shoulder pops, clicks, or has a catching sensation with specific movements (suggesting intra-articular pathology requiring assessment); or the postural correction program is not producing measurable progress after 8–12 weeks of consistent, correctly applied practice. A sports physical therapist or orthopedic PT with expertise in shoulder and cervical spine conditions can identify specific tissue restrictions, movement dysfunctions, and strength asymmetries that self-assessment may miss, and can customize the exercise prescription to the individual’s specific presentation in ways that generic programs cannot.
Postural Correction for Specific Sports: Athletes With Rounded Shoulders
Athletes whose sports involve repetitive overhead or forward arm movements — swimmers, cyclists, rock climbers, rowers — are at higher risk of rounded shoulder development from sport-specific muscle balance alterations alongside desk work. Swimming produces the highest pectoral and anterior deltoid loads of any common sport from the repeated pulling stroke, requiring even more aggressive posterior shoulder strengthening relative to pressing to offset the sport’s anterior loading. Cycling’s forward-flexed riding position produces both thoracic kyphosis and pectoral shortening from the sustained trunk flexion, making thoracic extension mobility work particularly critical alongside the shoulder correction exercises. Rock climbing produces forearm, bicep, and anterior shoulder dominance from the pulling demands of climbing — the specific correction for climbers adds external rotation emphasis and shoulder depression focus to address the specific muscle balance alterations their sport produces. Sport-specific postural correction recognizes that the exercises and stretches must address both the general rounded shoulder pattern and the sport-specific muscle balance alterations that compound the postural dysfunction — requiring greater emphasis on specific components of the general program based on which sport-related patterns are most dominant in the individual presentation.
Frequently Asked Questions About Fixing Rounded Shoulders
Can rounded shoulders be permanently fixed? Yes — rounded shoulders are a muscle balance and tissue length problem, not a structural skeletal deformity (except in rare cases of severe scoliosis or other structural abnormalities). Consistent corrective practice over months to years restores the muscle balance and tissue lengths that hold the shoulder in the corrected position automatically. The correction requires ongoing maintenance (continued training that avoids the extreme press dominance that created the problem), but true structural muscle balance correction is achievable for most people who apply the corrective program consistently.
Do posture corrector braces work? Posture corrector braces physically hold the shoulders in a retracted position through an external constraint, which can reduce discomfort during the wearing period and provide proprioceptive feedback about shoulder position. They do not correct the underlying muscle imbalance — and if used continuously as the primary correction strategy, they may actually reduce the stimulus for the inhibited posterior muscles to develop the strength needed to hold the correction without the brace, producing brace dependency rather than correction. The appropriate use of posture braces: as a proprioceptive cue during the early stages of correction, worn for 1–2 hours during focused work periods to heighten awareness, while the actual correction is built through the exercises and stretches. Not as a full-time correction device worn instead of the corrective exercise program.
How do I know if my rounded shoulders are improving? Progress indicators: the wall test — increasing ability to touch the back of the head, shoulders, and lower back to the wall simultaneously without lower back arching; the doorway stretch — deepening the comfortable stretch position as pectoral flexibility improves; single-leg shoulder blade positioning — the shoulder blades should be resting more flat and lower on the ribcage (less elevated, less winged) as lower trapezius strength improves; and subjective experience — reduced upper trap and neck tension, fewer tension headaches, and reduced shoulder impingement pain during overhead movements are reliable indicators of functional improvement even before dramatic visual postural change is evident.
Does massage help fix rounded shoulders? Massage therapy — particularly deep tissue massage and myofascial release targeting the pectoralis major and minor, upper trapezius, and levator scapulae — reduces trigger point activity and muscle tension in the hyperactive anterior shoulder muscles, producing temporary improved shoulder mobility and reduced pain. It does not produce the tissue length changes of consistent stretching or the muscle balance changes of strengthening. Its most valuable role in rounded shoulder correction is as a preparation for stretching — reducing the muscle tension that limits stretch depth immediately before a stretching session — and as symptom management during the months-long correction process when muscle tension and trigger point pain are limiting daily function and motivation.
The Connection Between Rounded Shoulders and Lower Back Pain
Rounded shoulders do not exist in postural isolation — the thoracic kyphosis and forward head posture that accompany rounded shoulders produce compensatory changes throughout the spinal chain that frequently contribute to lower back pain alongside the shoulder and neck symptoms. When the thoracic spine rounds excessively and the head translates forward, the lumbar spine must hyperextend to maintain the body’s center of mass over the base of support — producing the hyperlordotic (excessively arched) lumbar posture that loads the lumbar facet joints, compresses the posterior intervertebral disc annuli, and tightens the lumbar erectors and quadratus lumborum. Athletes with chronic lower back pain who also present with rounded shoulders frequently find that addressing the thoracic and shoulder posture reduces the compensatory lumbar loading that is the proximate cause of their back pain — the lower back problem is often the downstream consequence of the upper body postural dysfunction rather than an independent issue requiring separate management. The rounded shoulder correction program in this article, particularly the thoracic mobility and extension components, directly addresses the thoracic contribution to lumbar loading — making it relevant to lower back pain management alongside its primary application to shoulder and neck correction.
Using the NSCA’s Corrective Exercise Framework for Rounded Shoulders
The NSCA’s corrective exercise framework for postural dysfunction provides a structured approach to rounded shoulder correction that aligns with the program in this article: inhibit the overactive/short muscles through foam rolling and sustained static stretching, lengthen the overactive muscles through additional flexibility work, activate the underactive/inhibited muscles through isolated low-load exercises (face pulls, band pull-aparts, chin tucks), and then integrate the corrected movement patterns into functional exercise (rows, pull-ups, overhead press with corrected mechanics). This four-phase sequence — inhibit, lengthen, activate, integrate — is the evidence-based corrective exercise progression that converts isolated muscle function improvements into the integrated movement quality that makes the postural correction functional across all daily and athletic activities. Applying this framework to the exercises in this article: the SMR and stretching phases address inhibit and lengthen; the isolation exercises (band pull-apart, face pull, prone Y-T-W, chin tuck) address activate; and integrating these movement patterns into barbell rows, pull-ups, and overhead pressing with conscious attention to scapular mechanics addresses the integrate phase that completes the corrective exercise progression.
The most important single insight from this article for someone just beginning to address rounded shoulders: this is a muscle balance and tissue length problem with a known, well-researched solution, not a permanent structural condition that requires resignation or surgical intervention. Every person who applies the systematic program in this article consistently — stretching the short anterior muscles, strengthening the inhibited posterior muscles, modifying the daily environment that perpetuates the dysfunction, and sustaining the practice across the months the tissue adaptation requires — will experience progressive correction that compounds into the automatic, pain-free, functionally superior posture that is the goal. Start today; the correction timeline begins with the first consistent application of these practices.




